
Abstract
Introduction
Radiostereometric analysis (RSA) is an accurate and precise measurement tool of migration and rotation of implants. We investigated if early migration measured with RSA can be used to predict the risk of later aseptic loosening in acetabular revision surgery.
Patients and methods
A total of 312 patients who underwent acetabular revision surgery were followed by RSA measurements for 2 to 20 years. The endpoint was either re-revision due to aseptic loosening or loosening on last available radiographic examination. Cox regression model was used to evaluate the predictive value of early migration.
Results
A total of 16 acetabular cups were re-revised due to aseptic loosening and 7 unrevised cups were radiographically loose. Every mm of proximal migration 2 years postoperatively increased the risk of aseptic loosening by 37% (hazard ratio (HR) 1.37, 95% confidence interval (CI) 1.18-1.58). Adjusting for differences in base line demographics, bone defects and surgical techniques in a Cox regression model, risk of aseptic loosening with every mm of proximal migration was even higher (HR 1.94, 95% CI 1.34-2.82, p<0.001).
Conclusions
We found a strong relationship between early migration measured by RSA and risk of late aseptic loosening in acetabular revision surgery. Monitoring proximal migration with RSA should be considered as an essential step in quality assessment when new implants and novel techniques are introduced in acetabular revision surgery.
Introduction
The number of patients in need of a total hip arthroplasty is expected to increase during the next 2 decades (1). With primary hip implants becoming more prevalent the number of revision surgeries is expected to increase as well (1, 2), especially due to the increased use of hip replacement surgery in younger patients (2). In the Nordic countries aseptic loosening is the most common cause of hip implant failure necessitating revision surgery (3-4-5-6). Cup and/or liner revision is the most commonly performed revision procedure in the Nordic countries (5).
Radiostereometric analysis (RSA) was introduced by Göran Selvik in 1972 (7). This method enables accurate and precise measurements of rotation and migration of implants (8, 9). The migration pattern of implants used in primary total hip replacement has been evaluated by RSA measurements in multiple studies (10, 11). Proximal migration of the cup measured with RSA has proven to be a good predictive tool in primary acetabular failure (10). According to Pijls et al's meta-analysis every mm of proximal migration increases the risk of revision by 10% in primary cups (10). RSA has been suggested to be a helpful tool in the phased introduction of new implants in primary hip surgery (12). The failure rate in revision surgery is higher than in primary hip arthroplasties (13). Acetabular component failure is the most common cause for a second revision following revision surgery (13). New devices and surgical techniques are being introduced to optimise the outcome of acetabular revision surgery. Phased introduction of implants using RSA as a predictive tool will most certainly be of a benefit to patients (14) undergoing revision surgery. To our best knowledge there are no publications analysing the influence of migration measured with RSA on later risk of aseptic loosening in revised acetabular cups. In this analysis we studied the influence of early migration on risk of later aseptic loosening in acetabular revision surgery.
Patients and methods
All patients who entered this study were engaged in prospective studies at the Sahlgrenska University Hospital, Gothenburg, Sweden. The current study was approved by the regional ethical committee in Gothenburg, Sweden (reference number: 776-13). The inclusion criteria was cup revision performed during years 1993-2011 at Sahlgrenska University Hospital with a postoperative RSA examination and at least 1 further RSA measurement during the first 2 postoperative years. In patients operated bilaterally or several times during the study period the first hip and the first revision operated during years 1993-2011 was included in our analysis. The only exclusion criterion was the use of a metal reinforcement ring. Loosening defined as re-revision due to aseptic loosening, or radiological loosening at the last follow-up was used as outcome.
For the completion of the dataset all information available from the previous prospective studies was collected. The information from these studies was retrieved by preoperative and operative forms that were completed by the operating surgeon before and directly after the revision surgery. Data reported to the Swedish Hip Arthroplasty Registry (SHAR) were used to validate the forms. Since all patients in the study were continuously followed at our department we also collected missing data by performing case record studies, extra visits to the outpatient clinic and telephone calls to patients who did not want to or could not attend further follow up. By these measures we were able to gather complete data required for this analysis in all cases but 1. The end date of the present study was the 31st of December 2013.
Demographic and surgical data
During years 1993-2011, 352 hips in 312 patients were included in 5 different prospective studies at our institution. The first hip being revised during the aforementioned time period was included in this study. There were 125 men and 187 women. The majority of the patients underwent their initial hip replacement surgery due to primary osteoarthritis (n = 183). The remaining cases were grouped as secondary osteoarthritis (n = 129) of whom 39 cases had inflammatory disease, 16 cases femoral head necrosis, 27 cases were operated due to trauma and 47 cases due to previous childhood disease.
At the time of the index revision the mean age was 64 years (standard deviation (SD) 12.6) and the mean BMI was 25.8 (SD 4.0). In 162 hips the revision was performed on the right side and 150 cases were operated on the left side. The most common reason for revision was aseptic loosening (n = 247) followed by osteolysis (n = 23), deep infection (n = 23), dislocation (n = 5) and others (n = 14). In the majority of cases (n = 239) there were no previous acetabular revision surgeries performed, 56 cases had one previous acetabular revision before the index revision and the remaining 17 cases had undergone several previous revisions. The cup being removed was cemented in 170 cases and uncemented in 140 cases. There was 1 case in which a resurfacing prosthesis was removed and 1 in which an old ICHL double cup was extracted. The fixation method used during the index revision was uncemented in 244 hips and cemented in 68 cases. The most frequently used surgical approach was direct lateral (n = 200) followed by posterior (n = 86). The remaining cases were revised through a direct lateral or a posterior approach in conjunction with a trochanteric osteotomy. Bone grafting was used in 259 cases. In 14 cases detailed data on amount of bone graft used were missing. The senior author who had followed the majority of the patients from the start of this study approximated the amount of bone graft used in the aforementioned 14 cases after reviewing the case records and radiographs of the patients. In the remaining cases the mean amount of bone graft used was 55 ml (SD 53 ml).
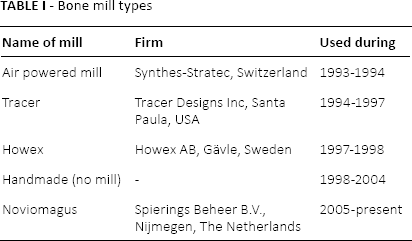
All bone grafts were made from fresh frozen femoral heads stored at our bone bank. Different bone mills were used (Tab. I). A bead insertion gun was used to insert 8-10 tantalum markers (Ø = 1 mm) in the cup or the liner and the same amount of markers (Ø = 0.8 mm) was inserted in the periacetabular bone for the RSA analysis. Until 2005 the cement used was Palacos® Heraeus Kulzer GmbH, Hanau, Germanywith gentamicin (Heraeus Kulzer GmbH, Hanau, Germany). Since 2005 Refobacin® bone cement or Refobacin® revision cement (AAP Biomaterials GmbH & Co. KG, Dieburg, Germany) was used in all cemented cups. Postoperative partial weight bearing for 3 months was prescribed until 1996. In 1996 the protocol changed to partial weight bearing 6 weeks postoperatively. Since 2011 immediate weight bearing as tolerated was allowed.
Bone mill types
Conventional radiography
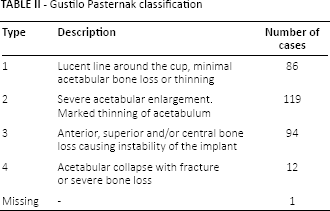
The bone defects were evaluated preoperatively in all cases by the operating surgeon, in 17 cases this information could not be retrieved. In these cases bone defects were assessed by the author reviewing the preoperative radiographs at the time the database was completed. The classification of Gustilo Pasternak was used (15) (Tab. II). In 1 case the classification could not be performed due to absence of preoperative radiographs and missing data in operative forms. Radiolucency at the last available radiographs of all cases were was assessed using the Charnley and DeLee classification modified by Hultmark (16, 17). Both anterior-posterior (AP) (regions 1-3) and lateral projections (regions 4-6) were evaluated. Occurrence of radiolucency was measured in all 6 regions by an independent observer (the 1st author). The extension of radiolucent lines between cup and bone was measured as the percentage of radiolucency in each of the 6 regions (17). Loosening was defined as complete (100%) radiolucency on either the AP or lateral view. Intra-observer validity was measured re-evaluating 45 randomly selected cases 2 weeks after the original assessment. A second observer (second author) evaluated the same 45 cases in order to assess the inter-observer validity. The intra- and inter-observer kappa values (18) regarding radiographic loosening were 1.00 and 0.87 respectively.
Gustilo Pasternak classification
Radiostereometric analysis
Radiostereometric analysis was performed postoperatively (1-7 days), at 6 weeks, 3 and 6 months and 1, 2, 3, 5, 7, 10, 13, 17 and 20 years after the revision surgery. The UmRSA software version 6.0 (RSA Biomedical Innovations, Umeå, Sweden) was used for all RSA measurements and calculations. All examinations were done with the patient in a supine position. The uniplanar technique with the calibration cage under the examination table was used (19, 20) and 3 generations of calibration cages were applied. During years 1993 to 1997 cage number 41 was used. In year 1997 the cage 43 was introduced and from 2013 cage 77 was utilised. The first change in year 1997 was initiated by the introduction of digital measurements and the second change (year 2013) was applied after the introduction of digital screens and use of new radiographic equipment.
Until 1997 analogue films were used. All measurements of these films were done on a digitsing table (21). Thereafter a digitised system with higher precision was introduced (9). The postoperative RSA radiographs were taken within 1 week after the operation. Evaluation was possible if at least 3 well-defined markers were identified in the acetabulum with a scatter corresponding to a condition number of less than 125 and marker stability up to 0,36 mm (20). The RSA-data of the previous prospective studies were gathered and updated. If an insufficient number of markers was available in the acetabulum the model-based technique was used to identify the position of the cup. This technique was only used in uncemented prosthetic designs. The accuracy of the model-based measurements performed at the Sahlgrenska University Hospital have been previously evaluated (22, 23) Comparison between the model based and regular RSA technique by linear regression model showed an adjusted r-square of 0.99 for proximal/distal translation with a 95% detection limit of 0.08 mm. The translation and rotation of the cup were analysed. The error of the RSA measurements, based on measurements of implant and bone markers was analysed in 20 double examinations. The 95% detection limit for rotation about the horizontal, longitudinal and sagittal axes was 0.45, 0.53 and 0.28 degrees respectively. The corresponding values concerning medial/lateral, proximal/distal and anterior/posterior translation were 0.40, 0.08 and 0.28 mm. The 2-dimensional migration was calculated by using the square root sum of proximal/distal and medial/lateral migration:

Statistical analysis
IBM SPSS 20 (IBM SPSS, New York, United States) was used for preparation of the data. The software R (The R Project for Statistical Computing) (24) was used for data processing. The hazard ratios for cup migrations during the first 2 years were calculated using Cox regression analysis without and with adjustment for differences in gender, age, method of fixation (cemented/uncemented), number of previous revisions, type of bone defect according to Gustilo Pasternak and amount of allograft used during revision surgery. Loosening as defined above was used as end-point. The hazard ratios (HR) from the Cox regression models are presented with 95% confidence intervals (CI) and p-values (p). Schoenfeld residuals (25) were used to ensure the proportional hazard assumption. Akaike information criterion (AIC) (26) and Akaike weights (27) were used to identify the best predictors among proximal migrations and 2 D migrations measured up to 2 years respectively. The baseline hazard and coefficients from the Cox regression analysis were used for calculations of revision probabilities at predefined time points when RSA recordings were performed.
Results
In total 33 cups were re-revised, 16 due to aseptic loosening. The mean time between the index revision and re-revision was 9.2 years (SD 4.0 years). In the non-revised cases radiographic loosening was detected in 7 cases after a mean of 13.5 years (SD 5.5). A total of 73 patients were deceased after a mean of 7.9 years (SD 4.2).
The mean proximal migration at 3 months, 6 months, 1 year and 2 years was 0.28 mm (SD 0.47), 0.38 mm (SD 0.83), 0.42 mm (SD 0.85) and 0.51 mm (SD 1.27) respectively. Corresponding values regarding 2-dimensional migration were 0.48 mm (SD 0.59), 0.67 mm (SD 1.11), 0.78 mm (SD 1.40) and 0.82 mm (SD 1.43). There was a higher mean proximal migration in patients being re-revised due to loosening or regarded as loose at the final follow-up (p≤0.03) (Fig. 1).
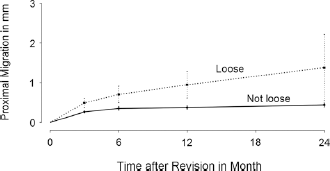
Mean proximal migration of the patients regarded as loose or becoming re-revised due to loosening was higher compared to patients without loosening (p≤0.03).
According to the Akaike weights, proximal migration and 2D migration values measured at 2 year postoperatively were the best predictor of late aseptic loosening (Tab. III).
Akaike and weighted Akaike values of adjusted Cox regression models with RSA measurements at different time points
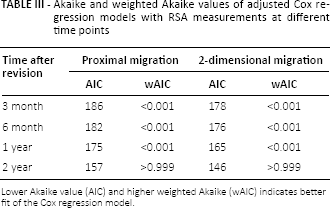
Lower Akaike value (AIC) and higher weighted Akaike (wAIC) indicates better fit of the Cox regression model.
Every mm of proximal migration 2 years postoperatively increased the risk of aseptic loosening with 37% (HR 1.37, 95% CI 1.18-1.58, p<0.0001). The corresponding value for 2-dimensional migration at 2 years was 39% (HR 1.39, 95% CI 1.20-1.60, p<0.001). After adjusting for differences in base line demographics, bone defects and surgical technique the Cox regression model revealed that for every mm of proximal migration at 2 years the risk of aseptic loosening almost doubled (HR 1.94, 95% CI 1.34-2.82, p<0.001) (Tab. IV). The corresponding risk increment for 2D migration measured 2 years postoperatively was 1.69 (95% CI 1.32-2.17, p<0.001). The probability of loosening increased with the degree of proximal migration measured at 2 years (Fig. 2). The correlation of 1, 2 and 3 mm proximal migration measured at 2 years and probability of loosening up to 20 years is illustrated in Figure 3.
Cox-regression analysis with loosening used as end-point
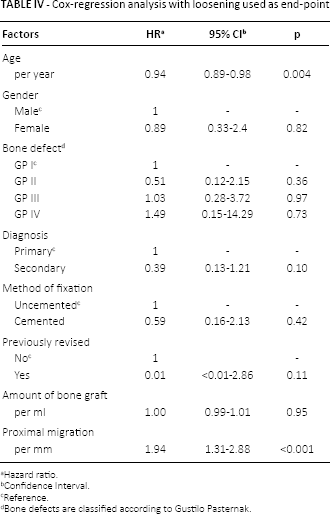
Hazard ratio.
Confidence Interval.
Reference.
Bone defects are classified according to Gustilo Pasternak.
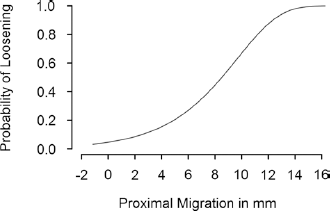
Probability of loosening as a function of the degree of the proximal migration measured at 2 years.
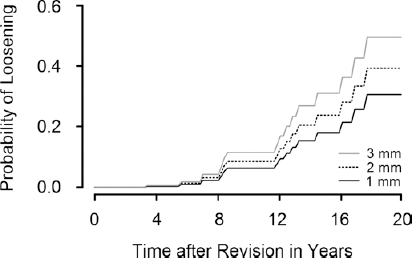
Probability of loosening for hips with a proximal migration of 1, 2 and 3 mm at 2 years postoperatively.
Discussion
We defined the relationship between acetabular component migration up to 2 years after the operation and risk of aseptic loosening in revision cups. We found a strong relationship between early proximal migration and 2D migration measured with RSA and risk of late aseptic loosening. Migration values recorded at 2 years were the best predictors.
Pijls et al, studied the correlation between early proximal migration and the risk of late aseptic loosening in primary cups (10). They concluded that every additional mm of proximal cup migration at the 2 year follow up, increased risk of aseptic acetabular loosening with 10%. According to our analysis the risk of aseptic loosening increases almost 2-fold with every mm of proximal migration and 1.7 times for every mm of 2D migration. These risk increments are much higher than the ones reported for primary cups (10). It could be hypothesised that the higher relative risks in our analysis is partly due to an increased early migration that occurs when bone impaction grafting is used. However, this hypothesis remains to be investigated. Another important difference is that Pijls et al. combined different patient cohorts and thus, did not study patients examined with RSA during a long period of time in order to analyse their long-term clinical outcome.
We included both cemented and uncemented revision cups in this analysis since different fixation methods have been used during the last 20 years at our hospital. According to Bolder et al (28) bone impaction grafting with a cemented socket has been described to be associated with some degree of proximal migration postoperatively due to remodeling of the allograft. In our analysis impaction grafting was used in both cemented and uncemented cups. Indeed all our cemented cups and majority of the uncemented designs were grafted. In the Cox regression model neither the amount of bone graft used nor the method of fixation had any influence on later risk of aseptic loosening (Tab. IV). It is unclear whether the uncemented designs, operated with bone impaction grafting, show the same amount of early proximal migration as cemented cup designs. We do believe that this issue needs further studies, preferably with a randomised design to arrive at more firm conclusions.
There are several limitations in this study. Firstly the proximal migrations could be either positive or negative. If the cup fails mainly by increase of inclination and rotation around a fulcrum close to its lateral edge, the cup center might migrate distally (negative value) followed by proximal migration when the cup dislocates out of the acetabulum. A high negative or positive migration rate is probably equally bad. We re-analysed our data with use of absolute values. In this analysis the predictive value of migrations was not altered significantly, probably because cases with distal cup migration (negative values) were few. Secondly there were some cases in which 1 or several migration values, during the first 2 years, could not be retrieved (n = 65). We therefore recalculated the hazard ratios with exclusion of these cases. In this analysis the 2-year migration data remained the best predictor with no major changes of the hazard ratios.
Based on the data available we conclude that early migration of a revision cup increases the risk of loosening. Proximal and 2-dimensional migrations measured with RSA are strong predictors for later aseptic loosening. We suggest that monitoring of cup migration with RSA should be considered as one of the first necessary steps in quality assessment when new implants and novel techniques are being introduced in acetabular revision surgery.
Footnotes
Acknowledgement
Bita Shareghi for her contribution in measuring majority of RSA investigations included in this study. Göteborgs Läkaresällskap (Gothenborg Medical Association) for the generous scholarships provided during 2014. Ingabrit and Arne Lundberg, Felix Neuberg research foundations and the Swedish Research Council for financial support.
Financial support: Financial support was received from Ingabrit and Arne Lundberg, Felix Neuberg research foundations and the Swedish Research Council.
Conflict of interest: Institutional research support for MM and JK from Zimmer Inc.