
Abstract
Patients undergoing total hip arthroplasty are increasingly younger and have a higher demand concerning hip range of motion. To date, there is no clear consensus as to the amplitude of the “normal hip” in everyday life. It is also unknown if the physical examination is an accurate test for setting the values of true hip motion. The purpose of this study was: 1) to precisely determine the necessary hip joint mobility for everyday tasks in young active subjects to be used in computer simulations of prosthetic models in order to evaluate impingement and instability during their practice; 2) to assess the accuracy of passive hip range of motion measurements during clinical examination. A total of 4 healthy volunteers underwent Magnetic Resonance Imaging and 2 motion capture experiments. During experiment 1, routine activities were recorded and applied to prosthetic hip 3D models including nine cup configurations. During experiment 2, a clinical examination was performed, while the motion of the subjects was simultaneously captured. Important hip flexion (mean range 95°-107°) was measured during daily activities that could expose the prosthetic hip to impingement and instability. The error made by the clinicians during physical examination varied in the range of ±10°, except for flexion and abduction where the error was higher. This study provides useful information for the surgical planning to help restore hip mobility and stability, when dealing with young active patients. The physical examination seems to be a precise method for determining passive hip motion, if care is taken to stabilise the pelvis during hip flexion and abduction.
Keywords
Introduction
Total Hip Arthroplasty (THA) aims to restore patient mobility by providing a pain-free and stable joint. An increasing number of younger and more active patients undergo THA for early onset arthritis (1, 2). Good function and longevity of a prosthetic hip depend on many inter-related factors. Suboptimal geometry, spatial positioning and orientation of implant components may contribute to early failures (3-4-5). Hip kinematics is also an important factor, since routine movements can cause impingements within the joint between both bony and prosthetic components, reducing the range of motion (ROM) and causing dislocations (6, 7).
The effects of prosthetic components positioning in resultant hip ROM, impingements and dislocation mechanisms have been previously documented (8-9-10-11). These studies were generally based on in vitro simulations of prosthetic models using simple, idealised kinematic sequences presumed to be representative of activities prone to implant failures. Unlike the works of Nadzadi et al (6) or Pedersen et al (7), too few studies have considered the use of more realistic subject's kinematic data as input for the simulation. Moreover, there exist no motion data matching the hip ROM of young patients in daily tasks, since previous simulation studies have focused on the prosthetic mobility of elderly patients. Nowadays, candidates for a THA are increasingly younger and more demanding on hip ROM, collecting data concerning this group is hence relevant for better surgical undertaking.
Another aspect that has caught our attention in this study is that patient care starts with correct physical examination and determining the patient's passive hip ROM is one of its key points. Usually, measurements of passive hip ROM are performed by clinicians using standard goniometers or inclinometers whose reliability has been well studied (12-13-14-15). Unfortunately, this process may lack precision because of movement of other joints around the pelvis (i.e., no direct access to the joint). It is also unknown whether the examiner's clinical experience plays a role in obtaining correct results. To our knowledge, assessing the accuracy of the physical examination as a method for determining the true passive hip ROM is little investigated. Some authors compared hip ROM measurements obtained with goniometer and electromagnetic tracking system (14) or optical motion capture (13), but these studies were affected by skin movement artifacts that could hinder accurate kinematic estimation with electromagnetic or optical motion capture systems (16). Therefore, research is still needed in order to attest the validity of the physical examination.
The purpose of this study was hence twofold: 1) to define in a precise way the necessary hip joint mobility for everyday tasks in young active subjects. These data would be then used in computer simulations of prosthetic hip joint 3D models to evaluate relative risk of impingement and loss of joint congruence during their practice; 2) to assess the accuracy of the passive hip ROM clinical examination as a method for setting the values of true hip motion.
In order to obtain accurate hip joint kinematic data, we performed a pilot study using a validated patient-specific technique coupling optical motion capture to magnetic resonance imaging (MRI) where skin movement artifacts are effectively tackled.
Materials and Methods
The present study included an MRI study and two different motion capture experiments. Experiment 1 - aimed at determining the hip ROM in everyday activities to be used in computer simulations of prosthetic hip models, while experiment 2 - intended to assess the accuracy of passive hip ROM measurements during clinical examination.
A total of 4 healthy young active participants (1 female, 3 males – 8 hips) were recruited from staff of the investigators’ research teams. Subject demographics are shown in Table I. Exclusion criteria were previous hip injuries, any kind of groin pain, hip surgery or contraindications for MRI. Institutional ethical approval and informed consent were obtained prior to data collection.
Subject demographics

MR Imaging and bone model reconstruction
The 4 volunteers were MRI scanned with a 1.5 T HDxT system (General Electric Healthcare, Milwaukee, WI, USA). A flexible surface coil was used and the images were acquired in the supine position. The imaging protocol was issued from a previous study (17) that allowed for the acquisition of images suitable for both radiologic analysis and bone model reconstruction. The region of interest of MRI datasets extended from the L4 vertebra to the knee. DICOM files of the scans were transferred to a personal computer and virtual 3D models of the hip joint were reconstructed thanks to custom-made segmentation software (18). MRI was privileged over Computed Tomography (CT) imaging, because it was not invasive and the software used has proven to be very accurate for the reconstruction of hip 3D bone models from MRI data (mean ± standard deviation error: 1.25 ± 1.0 mm) (18). As a result, patient-specific 3D models of the pelvis and femur were reconstructed for each volunteer.
A musculoskeletal radiology specialist evaluated all images to assess any bony abnormalities, such as hip dysplasia or cam/pincer morphology. The morphological analysis included the following radiographic criteria: acetabular depth (19), acetabular version (17), lateral center edge (CE) angle (20), anterior CE angle (20), femoral head-neck alpha angle (21), neck-shaft angle (22) and femoral neck anteversion (22). Measurements were performed on the MRI scans in accordance with the methods cited in the mentioned references. Thus, the acetabular depth and version were considered as normal when the value was positive. For the angles, they were considered as normal when included in the following ranges: lateral CE angle within [25°, 39°]; anterior CE angle within [25°, 39°]; alpha angle <55°; neck-shaft angle within [120°, 140°]; femoral neck anteversion <15°.
Motion capture experiment 1
To record the hip ROM in everyday life, the 4 participants were equipped with spherical retroreflective markers (Ø14 mm) placed directly onto the skin using double sided adhesive tape. A total of 2 clusters of 6 markers were placed on the lateral and frontal parts of both thighs; 6 markers were also stuck on pelvic anatomical landmarks (e.g., anterior superior iliac spines). Additional markers were distributed over the body (trunk, upper limbs, legs and feet) to confer a more complete visualisation from general to detailed.
Motion capture data from the participants were acquired during 5 activities: stand-to-sit, lie down on the floor, lace the shoes while seated and pick an object on the floor while sitting or standing. These movements were chosen, because they are known to be painful in case of hip disorders or prone to hip implants related complications (e.g., dislocation, impingements) (6, 7). Marker data were captured within a 108 m3 measurement volume (6 × 6 × 3 m) using 24 infrared cameras (Vicon MXT40S, Oxford Metrics, UK), sampling at 120 Hz. Participants were asked to perform each activity 3 times. For the activities requiring a chair, a standard 45 cm height stool was used to ensure that all pelvic markers were visible to motion capture cameras.
Motion capture experiment 2
In order to assess the accuracy of passive hip ROM measurement by physical examination, 2 orthopaedic surgeons with different levels of experience were involved in this experiment. Surgeon 1 (junior) had 2 years of clinical experience. Surgeon 2 (senior) had 12 years of clinical experience. Each examiner performed successively and in turn a measurement of hip ROM of the participants’ hips, while the motion of the subjects was simultaneously recorded using motion capture. Marker data were collected with the same motion capture system and the same markers set-up as those used for experiment 1.
Measurement of passive hip ROM was acquired according to the following sequences: 1) supine: maximal flexion, maximal internal/external rotation with hip flexed 90°, maximal abduction; 2) seated: maximal internal/external rotation with hip and knee flexed 90°. For all measurements, a hand held goniometer was used by the examiner to measure hip angles in those different positions according to the neutral zero method (23). Care was taken to stabilise the pelvis during passive motion to prevent overestimation of the motion values obtained. For both sequences, a standard hard table was utilised as an examination table in order to avoid movement artefacts occurring because of a mattress. The values obtained by the examiners were noted down to be later compared with the kinematic data computed from simultaneous motion capture.
Kinematic analysis
Marker data from motion capture experiments 1 and 2 were used to compute the 3D kinematics of the hip joint. The major drawback with optical motion capture systems is that markers are placed on the skin surface and move relatively to the underlying bone during activities with the deformation of the soft tissues. This represents an artefact and is usually referred to as soft tissue artefact (STA). STA has been proved to be the major source of errors in skin marker-based joint motion analysis (16). To solve this issue, we used a validated optimised fitting algorithm which accounted for STA and patient-specific anatomical constraints (24, 25). Indeed, computed motion was applied to the subject's hip joint 3D models reconstructed from their MRI data, which allowed accounting for the subject's anatomy and kinematic parameters (e.g., hip joint centre). The accuracy of this algorithm was 0.4, 0.59, 0.24 mm for medio-lateral, antero-posterior and proximo-distal translations, and 0.55°, 2.86°, 1.71° for flexion/extension, abduction/adduction and internal/external rotation, respectively. This provided sufficient accuracy for clinical use in the study of hip pathology and kinematics.
To permit motion description of the hip joint, local coordinate systems (Fig. 1) were established based on the definitions suggested by the International Society of Biomechanics (26) to represent the pelvic and femoral segments using anatomical landmarks identified on the subject's bony 3D models. The hip joint center was calculated using a functional method (27). For the motion capture experiment 1, the hip ROM was quantified for each participant and for all recorded daily activities. This was obtained given the computed bones poses from motion capture data by calculating the relative orientation between the pelvic and femoral coordinate systems at each point of the movement (25). This was finally expressed in clinically recognisable terms (flex/ext, abd/add and IR/ER) by decomposing the relative orientation into three successive rotations (28). It is important to note that the computations were performed independently of the major anatomical planes (i.e., sagittal, transverse, frontal planes). For the motion capture experiment 2, passive hip ROM recorded during clinical examination were quantified with the same method. Relevant angles were computed when the examiners were holding position of the lower limb in order to be compared with their measurements.
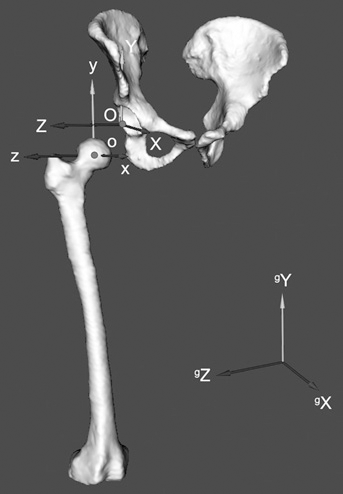
Reconstructed pelvis and femur bone models with pelvic (XYZ) and femoral (xyz) coordinate systems in relation to the global coordinate system (gX gY gZ). By computing the relative orientation of the femoral frame to the pelvic frame, the relative orientation between the pelvis and femur can be determined and decomposed into three successive rotations (flex/ext, abd/add and IR/ER).
Simulation of prosthetic hips
Movements recorded in the motion capture experiment 1 were applied to prosthetic hip models, in order to evaluate relative the risk of impingement and joint instability during everyday activities. To this aim, a 3D hip model with a prosthesis constituted by an acetabular cup of 48 mm and a femoral head of 28 mm diameter was created. Bone geometry was obtained from a 3D reconstruction of a pelvic CT in a young patient undergoing hip arthroplasty. Acetabular and femoral implants were modeled according to a standard commercial design (Medacta International, Castel San Pietro, Switzerland). The femoral component was implanted respecting the natural anteversion of the femur being parallel to the posterior cortex of the femoral neck. To explore the effect of acetabular component positioning, nine acetabular cup positions (combinations of 40°, 45° and 60° of inclination with 0°, 15° and 30° of anteversion) were chosen, including and extending beyond the conventional “safe zone” of 30°-50° of inclination and 5-25° of anteversion (29). Coordinate systems were established for the pelvis and femur based upon anatomical landmarks and definitions of the International Society of Biomechanics (26).
Simulation was executed with custom-made software that allows testing of the prosthetic hip model with real-time evaluation of impingement and joint instability (30). Hip angles (3 rotations) computed from motion capture data were first applied at each time step to the prosthetic model in its anatomical frame. Then, a collision detection algorithm (24, 25) was used to virtually locate any prosthetic or bony impingements. The impingement zone was denoted using a color scale (Fig. 2) of increasing contact (e.g., blue = no contact, red = highest contact) and its location documented based on a reference system dividing the acetabulum into 8 sectors (position 1, anterior; position 2, anterosuperior; position 3, superior; position 4, posterosuperior; position 5, posterior; position 6, posteroinferior; position 7, inferior; position 8, anteroinferior). When impingement occurred, the hip ROM was noted down. Moreover, femoral head translations were computed to evaluate the joint congruence. Since no loads were applied to the joint, the computed translations should therefore be viewed as only representative of joint instability or subluxation rather than dislocation. The reader can refer to the reference (30) for a more comprehensive description of the simulation technique. The 5 different daily activities (3 trials for each subject) were examined, thus a total of 60 simulations were performed for each cup position.
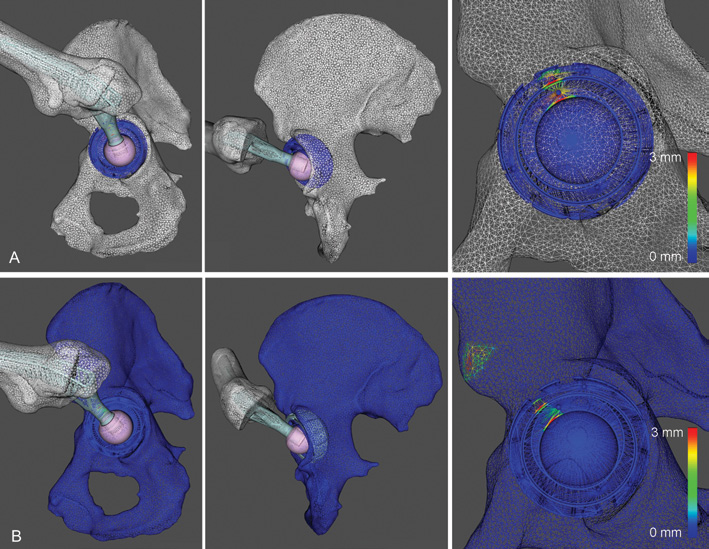
Visualisation of the impingement region during simulation (lateral and posterior views). The colours represent the area of increased contact (blue = no contact, red = highest contact).
Statistical analysis
We analysed all subject's hips according to the radiographic criteria. Maximum hip ROM from the 3 trials recorded in experiment 1 was determined for all participants and for all daily activities. For the simulations, we calculated the frequency of prosthetic and bony impingement and the distribution of the zone of impingement. We also computed the hip ROM and the amount and direction of subluxation when impingement occurred. We computed the errors made by the 2 examiners during the clinical exams recorded in experiment 2. The 2 different tests for measuring hip internal/external rotation (supine or seated) were also compared. For the comparisons between the goniometer and the motion capture measurements, Kolmogorov-Smirnov tests were first used to test for a normal distribution. Then, two-tailed Wilcoxon Signed-Rank tests were performed. A significance level was chosen at p<0.05. Descriptive statistics are presented as mean, range and standard deviations (SD) for each figure. The statistical software package R, version 3.1.1 was employed.
Results
Imaging data
According to the morphological analysis, the hips of the 4 volunteers did not present any cam or pincer morphology. No dysplastic hips, acetabular retroversion, femoral neck retroversion, deep acetabulum or abnormal offset of the femoral head-neck junction was noted. It was concluded that based on the radiologic criteria all 8 measured hips were morphologically normal. Table II summarises the results of our morphological analysis. For the femoral head-neck alpha angles, only the measurements in anterior and anterosuperior positions are reported, since they are the more significant.
Morphological analysis (n = 8) *
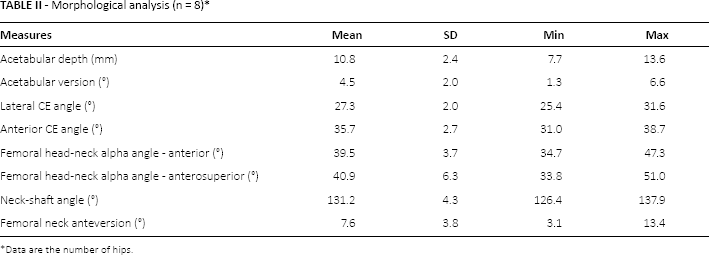
Data are the number of hips.
Motion data
As shown in Table III, daily activities involve intensive hip flexion. For all movements, a minimum of 95° hip flexion was required. Globally, the angles showed low standard deviations (range 3.6 to 12.2), suggesting that movements were performed similarly across subjects.
Maximum hip ROM (°) during everyday activities (n = 24) *
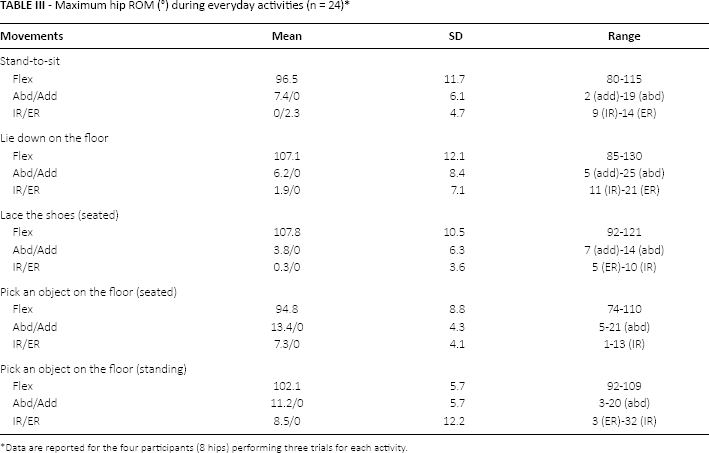
Data are reported for the four participants (8 hips) performing three trials for each activity.
Regarding the clinical examination, the errors made by the examiners varied in the range of ± 10°, except for the flexion and abduction where the errors were more significant (Table IV, flexion: mean 9.5°, range −7° to 22°, p = 0.058; abduction: mean 19.5°, range 8° to 32°, p = 0.014). No substantial differences between the errors made by the 2 examiners were noted (average error for each examiner: 7.4° vs. 8.4°). In Table IV, it is also interesting to note that examiners tended to overestimate flexion, abduction and internal rotation in supine position (positive mean values), while internal and external rotation tended to be slightly underestimated (negative mean values) in sitting position. For the differences between the hip internal/external rotations when measured in supine or sitting position, the results issued from both orthopaedists and motion capture measurements showed that the 2 tests did not yield similar results. Particularly, internal rotation was lower in supine than sitting for all measurements. Similarly, external rotation was always higher in supine than sitting.
Errors (°) made by the examiners and comparison between goniometer vs. motion capture measurements during clinical examination
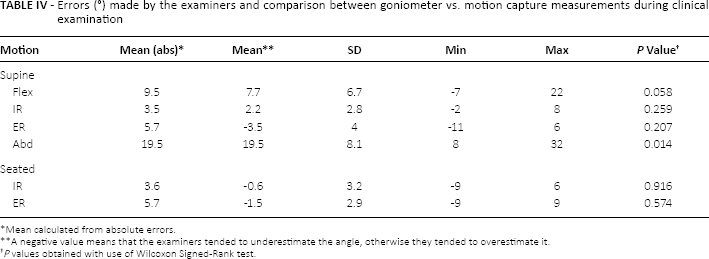
Mean calculated from absolute errors.
A negative value means that the examiners tended to underestimate the angle, otherwise they tended to overestimate it.
P values obtained with use of Wilcoxon Signed-Rank test.
Simulation data
Simulations showed collisions occurring at maximal ranges of motion in all cup positions (Tab. V). For all activities, cups with more inclination and anteversion encountered less impingement. ROM in flexion increased with increasing cup anteversion (e.g., 99° at 45°/0°, 101° at 45°/15°and 103° at 45°/30° in average during pick an object on the floor while seated). Regardless of the cup positions, most impingements were observed during lie down (83/108 trials, 77%) and lace the shoes (63/108 trials, 58%) which were the movements requiring the highest hip flexion. Both prosthetic and bony impingements were observed (Fig. 2), but prosthetic impingements were the most frequent (251 prosthetic impingements vs. 117 bony impingements out of 540 trials tested). Bony impingements between the medial corner of the femoral osteotomy and the anterior inferior iliac spine (subspine impingement) occurred during lie down (50%), lace the shoes (33%), pick an object on the floor while standing (25%), and their frequency was indifferent of the cup positioning. Concerning the location of impingements, they were located in either the anterosuperior or anterosuperior/superior area of the acetabulum (position 2 and 2/3 according to our documentation).
Impingement's location and occurrence, subluxation (mm) and hip Rom (°) when impingement occurred during daily activities. For each activity, the 3 trials of the 4 subjects were tested (n = 12)
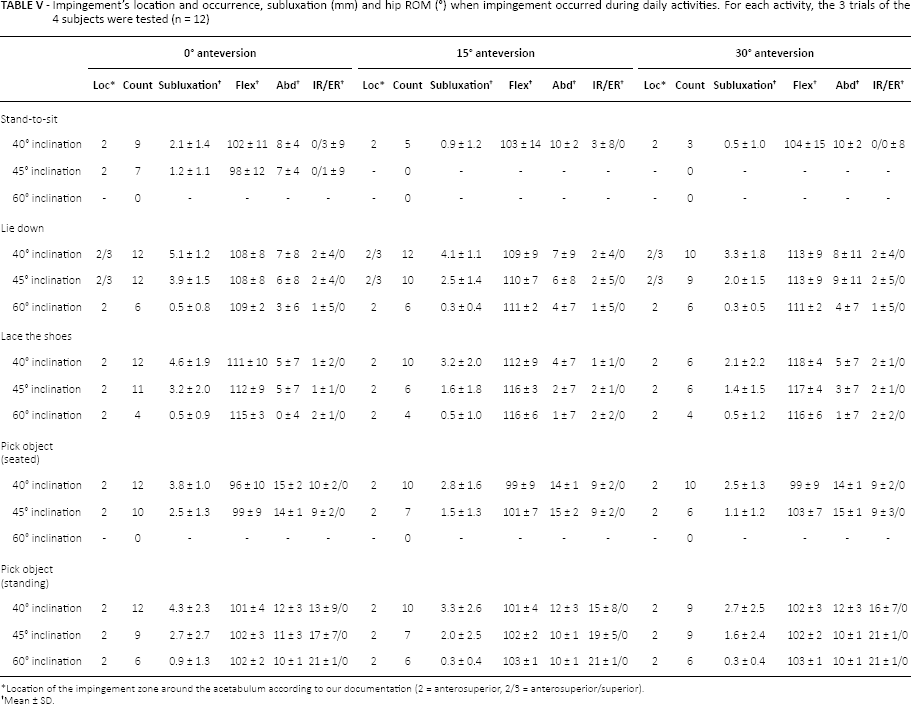
Location of the impingement zone around the acetabulum according to our documentation (2 = anterosuperior, 2/3 = anterosuperior/superior).
Mean ± SD.
Subluxations followed the same trend and were less important in cups with more inclination and anteversion (e.g., 5.1 mm at 40°/0°, 2.5 mm at 45°/15°and 0.3 mm at 60°/30° in average during lie down). For all cup positions and all activities, subluxations occurred in a posterior direction as a consequence of impingements.
Discussion
To date, there is no clear consensus as to the amplitude of the “normal hip”. Moreover, young patients are increasingly receiving surgical treatment for early onset hip disease. Current research related to THA generally focuses on the analysis of typical patients undergoing THA. Unlike previous works, we have presented an in-vivo study based on motion capture and MRI to accurately determine the ROM of the hip joint in young active subjects during daily activities. With the use of captured motion, computer simulations of prosthetic hip joint 3D models were performed to evaluate impingement and related joint instability during their practice. As far as we know, this is the first study that aims to objectively assess the accuracy of passive hip ROM measurements during physical examination.
Daily activities of a “normal hip” involve intensive hip flexion. For all movements, a minimum of 95° hip flexion was required, lacing the shoes and lying down being the more demanding. Abduction/adduction and internal/external rotation remained low and variable across subjects. As expected, the necessary hip joint mobility for everyday tasks in young active subjects was significant, which could explain why such motion can yield hip pain or possible early implant failure.
Regarding this latter aspect, simulations showed frequent impingements during movements occurring at maximal ranges of motion. No cup position was spared, but the ones with more inclination and anteversion encountered less impingement for all activities. This could be explained by the type of movements tested requiring a high degree of flexion, which renders the cups with less inclination and anteversion more favorable to abutment during such motion. We did not perform testing of movements of daily living requiring extension such as pivoting in a standing position or rolling over in bed, which could have yielded different results. It is also important to note that cups with more inclination or anteversion are often subject to greater stress concentrations and wear (7, 31). In terms of mobility, our data showed that the ROM in flexion increased with increasing cup anteversion, as previously noted (9, 10). Moreover, leaning over from a seated position to tie a shoe or lying down on the floor proved to be the most impingement-prone challenges. Concerning the location of impingement, they were mainly located in the anterosuperior area of the acetabulum leading to posterior subluxation. These instability patterns were consistent with previous works (7, 10). Eventually, both prosthetic and bony impingements were observed. The frequency of bony impingements was indifferent of the cup positioning. This may be due to the geometry of the bones used in the simulation with the high amplitude of movements tested which render the conflict inevitable whatever the position of the cup.
Concerning physical examination, the results showed that the errors made by the 2 examiners were acceptable for internal/external rotation, but were quite significant when evaluating passive flexion and abduction. For these last 2 measurements, virtual simulations of the process revealed interesting motion trends of the pelvis during the exams. During flexion, a posterior rotation of the pelvis in the sagittal anatomical plane was observed. This movement was accompanied by a slight flexion of the hip joint that hence followed the alignment of the acetabulum. During abduction, a medial rotation of the pelvis in the frontal anatomical plane was observed. These motion patterns could explain why examiners overestimated the values of these 2 measurements by ignoring subtle motion of the pelvis. Regarding the differences between the 2 tests for measuring hip internal/external rotation, internal rotation was lower in supine than sitting, while external rotation was higher in supine than sitting. The errors made by the examiners were equivalent in both tests. Therefore, both tests should be performed when examining the hip joint since the results observed express different values of pelvic position variation. The examiner's experience was also not found to be a determining factor.
Several study limitations need to be stated: firstly, the collection of motion data was based on a small number of participants. This work is part of a larger research project that aims to improve the pre-operative planning for THA by including a dynamic simulation of the prosthesis using motion data in everyday life of representative subjects. Our goal was to perform a pilot study to attest the validity of the methods developed before performing clinical studies with patients undergoing THA. Secondly, potential sources of errors should be mentioned such as the 3D bone reconstruction from MRI data (error ≈ 1.25 mm) and the kinematics computation from motion capture data (translational error ≈ 0.5 mm, rotational error <3°). Thirdly, our prosthetic joint simulation ignores the contributions of loads and soft tissue structures around the joint that could play a role in the impingement and dislocation mechanisms. Finally, the radiological analysis for hip abnormalities was based on native hip MRI (reliability of the findings estimated at 65%) and not MR arthrography that may offer better definition of intra-articular pathology.
Daily activities involve important hip flexion that could expose the prosthetic hip to impingement and subluxation. This information should be considered in the surgical planning and prosthesis design when restoring hip mobility and stability, particularly when dealing with young active patients. The clinical examination seems to be a precise method for determining passive hip motion, if extra care is taken to stabilise the pelvis during flexion and abduction to prevent overestimation of the range of motion. Further studies are required before attesting to the accuracy of this test.
Footnotes
Acknowledgments
We would like to thank Dr. Placido Bartolone for his participation in the motion capture experiment #2 and Matteo Ponzoni for his help in the preparation of the different implant configurations.
Financial support: This research work was supported by the “MyHip: Patient-Specific Pre-operative Planning and Intra-operative Surgical Guidance for Total Hip Arthroplasty” project funded by the Swiss Commission for Technology and Innovation (CTI n° 13573.1 PFFLE-LS).
Conflict of interest: None.