
Abstract
Introduction
Bone cement for fixation of prostheses, comorbidity and age have been previously shown to be associated with increased relative risk of mortality within the first day of surgery. However, the proportion of mortalities associated to each of these exposures is not adequately expressed by relative risk estimates.
Materials and methods
The attributable fraction (AF), i.e. the fraction of diseased individuals attributed to a given risk factor, was estimated for cemented fixation of hip prostheses in the elderly (>65 years) with a hip fracture. Dementia, symptomatic comorbidity (American Society of Anesthesiologists (ASA)≥ 3), old age (≥85 years), male gender, and a delay of 24 hours or more from fracture to operation were considered as additional risk factors for a fatal outcome in close proximity to surgery.
Results
In the entire study population (n = 11210), the unadjusted and adjusted population AFs of cemented fixation on mortalities within the first day after surgery were 0.58 (95% CI 0.28-0.76) and 0.59 (95% CI 0.29-0.76), respectively. Symptomatic comorbidity and old age as risk factors had population AFs of 0.71 (95% CI 0.51-0.83) and 0.55 (95% CI 0.39-0.67), respectively. Male gender, dementia and time from fracture to operation all had considerably lower population AFs.
Conclusions
The estimated AFs on perioperative mortality in hip fracture patients treated by hemiarthroplasty showed that about half of the mortalities within the first day of surgery could be associated with the use of bone cement.
Introduction
Surgical treatment of hip osteoarthritis with a cemented prosthesis has been linked to cases of fatal outcome in close proximity to surgery. This has often been referred to as “the bone cement implantation syndrome” (1, 2). Neurodepressive, vasoactive, cytotoxic and procoagulant events directly or indirectly caused by methylmethacrylate monomer have been demonstrated in laboratory and human studies (3-4-5-6-7-8-9-10). Thus, the monomer may trigger cardiorespiratory and vascular instability through a multitude of pathological reactions that occasionally lead to a fatal outcome.
We conducted an epidemiological study on perioperative mortality as an outcome in 11210 hip fracture patients treated with cemented or uncemented hemiarthroplasties (11). The risk ratio (RR) of mortality within the first day of surgery was increased in the cemented group (RR 2.9, 95% CI 1.6-5.2) adjusted for age, gender, cognitive impairment and symptomatic comorbidity. This was in accordance with another register-based study (12).
The effect of risk factors on mortality is typically expressed as an odds ratio, risk ratio or hazard ratio. These effect measures are derived from logistic, Poisson or Cox regression. However, using only these relative risk estimates does not adequately express the clinical and public health implications of a given risk factor. It is often more useful to calculate the proportion of subjects in a population with a fatal outcome which could have been avoided if they had not been exposed to a given risk factor. This is accomplished by estimating the attributable fraction (AF), which is a method used commonly in public health epidemiology (13).
The aim of this study was to estimate the proportion of perioperative mortalities attributed to the use of cemented implantation in hip fracture patients treated with hemiarthroplasties and compare it with other risk factors such as dementia, old age, male gender and time from fracture to surgery.
Methods and Methods
Patient characteristics
The Norwegian Hip Fracture Register (14) contains data from all hospitals in Norway on surgical treatment of hip fracture patients. Data on hip fracture patients from this register are given in Table I and include the time period January 2005 – December 2010. A total of 12394 patients were extracted of which 1184 had missing data, leaving 11210 patients available for statistical analysis (11). There was a significantly higher proportion of patients with dementia in the uncemented compared with the cemented group (p=0.031) and a significantly higher proportion of patients with 24 hours or more from fracture to operation in the cemented compared with the uncemented group (p<0.001). There were no statistically significant differences between patients with cemented or uncemented fixation for ASA score, age and gender.
PATIENT CHARACTERISTICS ACCORDING TO FIXATION METHOD
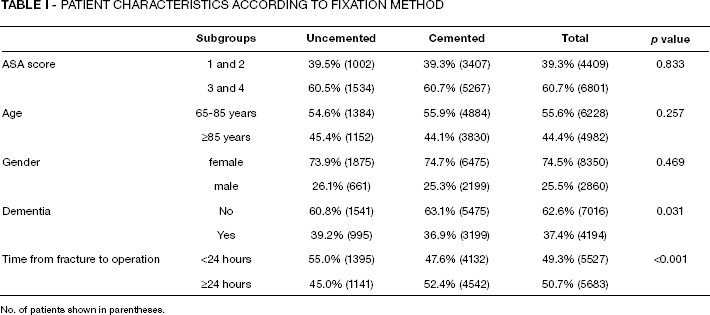
No. of patients shown in parentheses.
The date of death was collected from “Statistics Norway” covering the period up to 48 hours after operation, i.e. the day of surgery and the following day.
Statistical analysis
Baseline characteristics between the two groups were described with percentages and number of patients and tested with the chi-square test for categorical data.
The population AF is epidemiologically interpreted as the fraction of cases in the study population that can be attributed to given exposures (15, 16). It can be expressed both as an unadjusted estimate, i.e. an estimate that is unadjusted with respect to other risk factors, or as an adjusted estimate, i.e. an estimated that is adjusted with respect to other risk factors of interest. This epidemiological concept has been developed further to assess elimination of risk factors in sequential order and thereby calculating the corresponding average AF (17). A comprehensive description of the statistical and epidemiological properties of AFs has been provided by Eide and Gefeller (18).
All statistical analyses were conducted using Stata version 12 (College Station, Texas, USA). The unadjusted and adjusted RR of mortality within the first day after surgery were estimated using Poisson regression. Unadjusted and adjusted AFs with 95% CI were estimated using the punaf-package downloaded from Boston College Statistical Software Components (SCC) archive (19). Unadjusted AFs were also calculated using the cs command in Stata 12 (20).
Results
Fraction of perioperative mortalities attributed to cemented fixation and other risk factors
Mortality rate (MR) within the first day after surgery together with unadjusted and adjusted RRs for cemented fixation, ASA score, age, gender, dementia and time from fracture to operation are given in Table. II. The unadjusted and adjusted (for the other risk factors given in Tab. II) RR of cemented fixation were similar (RR 2.8, 95% CI 1.6-5.1 and RR 2.8, 95% CI 1.5-5.1, respectively). In the study population of 11210 patients, 128 died within the first day after surgery (MR 11.4 per 1000 persons). The unadjusted and adjusted population AF of cemented fixation on perioperative mortality were 0.59 (95% CI 0.29-0.76) and 0.58 (95% CI 0.28-0.76), respectively. Symptomatic comorbidity (ASA≥3) or old age (≥85 years) gave adjusted population AF of 0.71 or 0.55, respectively. Male gender, dementia and time to operation had statistically insignificant adjusted population AF of 0.02, 0.09 and 0.12, respectively (Tab. II).
MORTALITY RATE PER 1000 PERSONS (MR), UNADJUSTED AND ADJUSTED RISK RATIO (RR) AND ATTRIBUTABLE FRACTION (AF) FOR MORTALITY WITHIN ONE DAY AFTER HIP FIXATION SURGERY
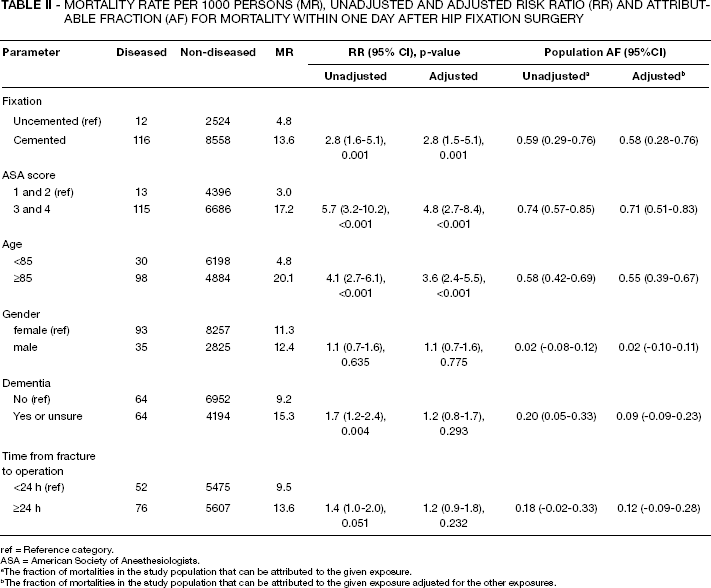
ref = Reference category.
ASA = American Society of Anesthesiologists.
The fraction of mortalities in the study population that can be attributed to the given exposure.
The fraction of mortalities in the study population that can be attributed to the given exposure adjusted for the other exposures.
Sequential and average AFs
The estimated sequential AF of three selected risk factors on perioperative mortality are given in Table III. Given a scenario where cemented fixation was eliminated as the first intervention in the study population of hip fractures; the corresponding sequential AF was 0.58. This is the same as the adjusted population AF of cemented fixation in Table II. If cemented fixation followed elimination of 24 hours or more from fracture to the operation (i.e. late operation), its sequential AF was 0.51. On the other hand, if symptomatic comorbidity was eliminated first, cemented fixation had a sequential AF of 0.17.
SEQUENTIAL ATTRIBUTABLE FRACTIONS (AFS) OF ELIMINATING CEMENTED FIXATION (CEMENT), 24 HOURS OR MORE FROM FRACTURE TO OPERATION (LATE OPERATION) OR SYMPTOMATIC COMORBIDITY EXPRESSED AS ASA ≥3 (HIGH ASA) ALL POSSIBLE SEQUENTIAL ORDERS
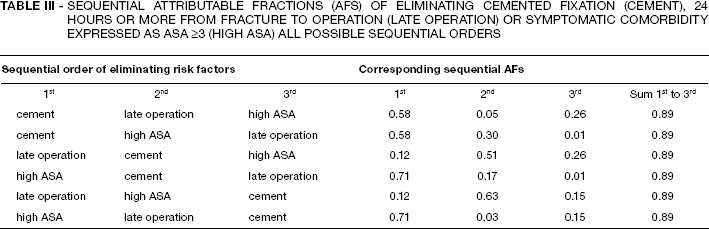
The corresponding average AFs of cemented fixation on perioperative mortalities was 0.36 (i.e. the mean of all the sequential AFs of cement fixation in Tab. III). For symptomatic comorbidity and late operation, the average AFs were 0.48 and 0.06, respectively.
Discussion
The baseline characteristics of the uncemented and cemented patients were rather similar and the unadjusted and adjusted RR of cemented fixation on perioperative mortality did not substantially differ. Therefore the effect of cemented fixation seems minimally confounded by the other investigated risk factors. In our study population of 11210 patients, the adjusted population AF of cemented fixation was 0.58. The epidemiological interpretation was that 58% of the perioperative mortalities of surgically treated hip fracture patients were associated with the use of cemented fixation. Expressed in another way, 6.6 immediate mortalities (i.e. 58% of the total MR of 11.4) per 1000 operated persons could theoretically have been avoided if nobody had received bone cement in the entire study population. The relative risk effect of cemented fixation on perioperative mortality did not substantially differ between patients with or without symptomatic comorbidity (results not shown), but the overall higher mortality among the frailer patients causes cemented fixation to have a larger public health impact compared with its effect among the healthier ones.
The average AF of cemented fixation and symptomatic comorbidity on perioperative mortalities was 0.36 and 0.48, respectively. This measure represents the expected effect of removing a given exposure after a random selection of other exposures has already been removed (18). Based on these calculations, if hip fracture treatment with cemented prostheses had been avoided, it would have had about 75% of the effect on perioperative mortality as eliminating symptomatic comorbidity in this study population.
Our results seem robust and show that more than half of the mortalities within the first day of surgery after hip prosthesis implantation are associated with the use of bone cement. This is in accordance with Costain et al (12) who found significantly increased mortality on the first postoperative day when cement was used, but a reversed risk in one-week data. A study from the Nation Hip Fracture Database showed a lower mortality at discharge with cemented fixation (21). Their measure on mortality included all deaths, from surgery to discharge and did not specify deaths the day of surgery and the first postoperative day.
The strength of our study was the large register-based cohort where mortalities within the first day of surgery were verified. Deaths that occurred 48 hours after surgery are likely to be due to other risk factors than a direct effect of bone cement (22) and were therefore not investigated in this study. Our findings are in accordance with case reports (23, 24), small clinical cohorts and trials (25, 26) and a number of ex vivo and in vivo pathophysiological studies performed on cells, animals and humans. These investigations examined the toxic effect and the additive mechanical trauma to the bone marrow caused by bone cement, which is historically referred to as “the bone cement implantation syndrome” (27). Our epidemiological study assessed the fraction of perioperative mortalities attributed to application of bone cement in hip fracture patients treated with hemiarthroplasties. It strongly indicated that bone cement is related to the majority of deaths occurring during and soon after surgery.
To our knowledge, the effect of cemented anchoring on mortality has not previously been assessed using the methodology of AFs. This methodology is commonly used in public health epidemiology to calculate the number of individuals in a population with disease that could have been avoided if they had not been exposed to some harmful agent, or if they had been treated differently (18). These calculations assess its impact from a public health perspective in a more informative way than relative risk estimates. In this study we showed that AF is a useful statistical and epidemiological tool in orthopaedics that can consolidate data in an alternative way to relative risk estimation.