
Abstract
Objective
This study examines the lipid profile change produced in response to tamoxifen (TAM) treatment, and its possible relationship with both apolipoprotein E genotype and menopausal state in patients with breast cancer. Methods: Blood samples were collected from 86 Spanish women with breast cancer before initiating TAM treatment and in the following 6, 12 and 18 months of treatment. Plasma lipid levels (total cholesterol, triglycerides, HDL-cholesterol and LDL-cholesterol) were determined using an automatic analyzer. Genotypes for apolipoprotein E (ApoE) were identified by PCR-RFLP using the HhaI enzyme.
Results
In all patients, significant reductions in total cholesterol and LDL-cholesterol concentrations and a significant increase in triglyceride concentrations were observed after 6, 12, and 18 months of TAM treatment compared to baseline (p<0.01 for each time point). In the subset of APOE4-negative patients, triglyceride concentrations also significantly increased after 6, 12, and 18 months of treatment (p=0.019, p=0.045, p=0.001, respectively), while APOE4-positive patients showed no significant lipid changes at 12 and 18 months. However, after 18 months of TAM treatment the overall triglyceride concentrations had risen by 24.75% in APOE4-negative patients vs 29.9% in APOE4-positive patients. In postmenopausal women, significant reductions in total cholesterol, LDL-cholesterol and LDL/HDL ratios were observed at each time point (p<0.020 for each).
Conclusions
TAM treatment induced similar plasma triglyceride increases in patients with positive or negative APOE genotype. Compared to premenopausal patients, postmenopausal breast cancer patients showed a more beneficial lipid profile change in response to treatment.
Introduction
Tamoxifen (TAM) is widely used as an adjuvant in breast cancer (BC) treatment because of its antiestrogen effects. TAM therapy has been described as cardioprotective due to its beneficial effects on lipoprotein metabolism, reducing plasma levels of total cholesterol (TC) and LDL-cholesterol (LDL-C) (1). In addition, TAM therapy has been linked to increased levels of apolipoprotein A-1 and reduced levels of apolipoprotein B-100, both considered reliable markers of cardiovascular disease (2). The use of TAM has also been related to elevated plasma triglyceride (TG) levels as an important adverse effect (3, 4).
The role of the apolipoprotein E (ApoE) in lipid metabolism has been extensively investigated. It is well known that ApoE is a constituent of very low-density lipoproteins and high-density lipoproteins and acts as a ligand to hepatic receptors (5, 6). The 3 most common isoforms of the ApoE protein in humans are E2, E3 and E4, which are encoded by the corresponding alleles ∊2, 3 and 4 (5, 6). The presence of some ApoE isoforms, such as ApoE4, determines faster chylomicron clearance and reduced plasma TG levels, whereas the ApoE2 isoform has been associated with increased plasma TG levels due to its minimal receptor binding activity (7). Several studies have addressed whether the APOE genotype affects the link between serum lipids and breast cancer risk. For instance, Moysich et al (8) reported a relationship between high plasma TG levels and cancer risk modified by the APOE genotype and Porrata-Doria et al (9) observed an increased prevalence of the APOE4 allele in women with early-onset BC. However, the effects of TAM on lipid profiles according to ApoE phenotype have been scarcely addressed and results so far have been controversial. Liberopoulos et al (10) noted that the levels of cardiovascular disease markers and TG responded more favorably to TAM treatment in APOE4-negative than APOE4-positive Greek postmenopausal women with BC. In contrast, Chang et al (11) reported that Taiwanese BC APOE4-positive patients showed significantly lower plasma TG levels when receiving TAM therapy.
The present paper describes the changes produced in plasma lipid profiles in response to TAM treatment in 86 Spanish women diagnosed with BC. The response produced was correlated with both APOE genotype and menopausal state. This descriptive study was designed to examine whether a specific menopausal state or being carrier of a given APOE allele could lead to favorable or harmful changes in the plasma lipid profiles of BC patients during TAM treatment.
Materials and Methods
Patients
The study participants were recruited among Caucasian Spanish women who had been recently diagnosed with BC at the Fundación Tejerina-Centro de Patología de la Mama (Madrid, Spain). Eighty-six premenopausal and postmenopausal patients were enrolled after undergoing primary surgery, radiation, and adjuvant chemotherapy and started on 20 mg/day of TAM as standard adjuvant therapy. All patients had normal lipid profiles before initiating TAM. Patients were excluded if they had one of the following conditions: diabetes mellitus, liver or renal failure, alcoholism, hypothyroidism or primary hyperlipidemia. Four venous blood samples were collected from each women at different time points: just before the start of TAM therapy and at 6, 12, and 18 months after treatment onset. Ten milliliters of heparin plasma were separated by centrifugation and immediately stored at -20°C until analysis. Additionally, 1 mL of an EDTA blood sample was obtained for subsequent DNA extraction and genotyping. The study protocol was approved by the review board of the Hospital de Getafe (Madrid). Written informed consent to participate in the study was obtained from all patients.
Lipid profiles
Plasma levels of TC, TG, HDL-cholesterol (HDL-C) and LDL-C were determined in triplicates at each of the 4 time points (at baseline and after 6, 12, and 18 months of TAM treatment) using an automatic Cobas Integra® 400 plus analyzer (Roche, Madrid, Spain).
DNA analysis
Genotyping was performed at the Molecular Biology Laboratory of the Universidad Europea de Madrid. Genomic DNA was isolated and purified from peripheral whole blood samples using standard phenol-chloroform procedures. APOE polymorphisms were identified by PCR using the following primers: forward, 5′-CGGGCACGGCTGTCCAAGGAG-3′; reverse: 5′-CACGCGGCCCTGTTCCACCAG-3′, as described by other authors (12). Samples scoring positive were digested with the HhaI restriction enzyme (New England Biolabs®, Ipswich, England) for 16 hours at 37°C. Digestion products were separated on 10% polyacrylamide gel using the pUC19 DNA/MspI (HpaII) marker (Fermentas PureExtreme®, Thermo-Fisher Scientific, USA): 2 (91 bp, 83 bp, and 33 bp), 3 (91 bp, 48 bp, and 33 bp) and the 4 allele (72 bp, 48 bp, and 33 bp).
Study design
The study design was retrospective and stratification by both APOE genotype and menopausal state was performed. Samples were collected from January to June 2009.
Statistical analysis
Allele and genotype frequencies and their consistency with Hardy-Weinberg equilibrium were estimated using the Genepop software (http://genepop.curtin.edu.au/). TAM effects on plasma TC, TG, LDL-C, HDL-C and LDL/HDL ratio were assessed using a paired t-test according to APOE genotype (E4-positive vs E4-negative) and menopausal state (premenopausal vs postmenopausal). All statistical tests were performed using SPSS software (version 20.0 SPSS, Chicago, IL). Significance was set at p<0.05.
Results
The cohort examined comprised 86 Spanish patients with BC with a mean age of 49.1 years (SD=9.7, range 19 to 76). Overall, 69% of the patients were postmenopausal and 31% premenopausal.
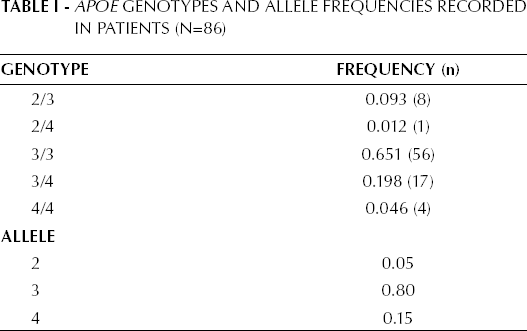
APOE genotypes and allele frequencies for the 86 patients are provided in Table I. Patients were stratified according to APOE genotype into the following subsets: 22 APOE4-positive (2/4, 3/4 and 4/4) and 64 APOE4-negative (2/3 and 3/3). The prevalence of APOE4 carriers in this sample was 25.6%, which is similar to that reported for other Caucasian populations (9).
APOE Genotypes and Allele Frequencies Recorded in Patients (N=86)
Plasma lipid changes recorded at baseline (before TAM treatment) and at 6, 12, and 18 months of treatment are shown in Table II. Significant reductions in TC and LDL-C levels were observed after 6, 12, and 18 months of TAM treatment (p<0.001 in each case, Tab. II), while plasma TG concentrations increased significantly after 6 months (p=0.002), 12 months (p=0.007) and 18 months (p<0.001) (Tab. II).
Changes in Plasma Lipid Levels (Mean and Standard Deviation) Produced in Response to TAM Treatment in Patents with Breast Cancer (N=85)

P values correspond to differences with respect to baseline (pretreatment).
According to the APOE4 genotype, plasma TG concentrations rose significantly in response to 6, 12, and 18 months of treatment in APOE4-negative patients (p=0.019, p=0.045, p=0.001, respectively, Tab. III), while no significant changes were recorded at 12 and 18 months (p=0.060 and p=0.054, respectively) in APOE4-positive patients. However, it should be noted that by 18 months of treatment, the overall TG concentration increase produced in APOE4-negative patients was 24.75%, compared with 29.9% in the APOE4-positive patients. Plasma TC and LDL-C levels underwent significant reductions in both APOE4-positive and APOE4-negative patients in response to 12 and 18 months of treatment (Tab. III). However, APOE4-negative patients showed significant reductions in the cardiovascular risk factor LDL-C/HDL-C after 6, 12, and 18 months of TAM treatment (p<0.01 for each time point, Tab. III), while such a reduction was only recorded after 18 months of treatment in the APOE4-positive patients (p=0.023, Tab. III).
Changes in Plasma Lipid Levels (Mean and Standard Deviation) Produced in Response to Tam Treatment in Patients with Breast Cancer Stratified by APOE4 Genotype (N=85)

P values correspond to differences with respect to baseline (pretreatment).
When patients were stratified by menopausal state, we observed that the decrease in TC and LDL-C levels produced by TAM treatment was more pronounced in postmenopausal women, with differences being significant at each time point (p<0.02 in each case, Tab. IV). With regard to the TG levels, a similar increase was observed in both pre and postmenopausal patients (Tab. IV), while the LDL-C/HDL-C ratio decreased significantly in the postmenopausal patients yet remained unchanged in premenopausal women (Tab. IV).
Changes in Plasma Lipid Levels (Mean and Standard Deviation) Produced in Response to tam Treatment in Patients with Breast Cancer Stratified by Menopausal State (N=84)

P values correspond to differences with respect to baseline (pretreatment).
Discussion
TAM is widely used as adjuvant therapy in early hormone receptor-positive BC. Several studies indicate that TAM has beneficial effects on lipoprotein metabolism in that it induces significant reductions in plasma TC and LDL-C levels (1) as well as in C-reactive protein, ApoA levels and the ApoB/ApoA ratio (13). However, there are also data suggesting that TAM treatment elevates plasma TG concentrations, thus likely increasing the risk of coronary heart disease (3, 4, 14). According to Liu et al, by reducing the daily TAM dose from 20 mg to 10 mg, the marked hypertriglyceridemia that occurs in some patients during TAM treatment may be improved (3).
Correlations between APOE polymorphisms and genotypes and the responses shown by plasma TG levels to diets or TAM treatment have also been described. Liberopoulos et al proposed that hypertriglyceridemia resulting from TAM therapy only occurs in APOE4 carriers (10). In contrast, Hozumi et al suggested that the TG increase observed during TAM therapy may affect every APOE genotype (14). Here, we observed significant increases in TG levels in APOE4-carrying patients after 6, 12, and 18 months of TAM treatment. However, our results for APOE4-negative patients were not conclusive since, despite a significant TG increase only observed at 6 months, by 18 months the overall increase was 24.75% versus a 29.9% increase in APOE4-positive patients. Chang et al described that the APOE4 allele has a beneficial effect on plasma TG levels in BC patients receiving TAM therapy based on their observation of a significant decrease in TG levels in APOE-positive patients (11). We were unable to confirm the minimal receptor binding activity and reduced clearance of TG attributed to the APOE2 allele (7), due to the low number of patients featuring the allele 2 (only 9 out of 86).
Our results indicate a significant decrease in TC and LDL-C levels induced by TAM treatment in postmenopausal women, whereas for TG levels a similar increase was observed in both pre and postmenopausal patients (Tab. IV). Because of a likely reduction in the risk of cardiovascular disease, TAM therapy might therefore benefit postmenopausal more than premenopausal women. The significant reduction in TC and LDL-C levels observed here in response to TAM treatment in postmenopausal women has also been described by others (15, 16). Further, a significantly lowered LDL-C/HDL-C ratio, a good predictor of cardiovascular events, was observed in the postmenopausal patients examined here, which is also in agreement with previous findings (10). In contrast, this effect was not detected in our subset of premenopausal women (Tab. IV). Accordingly, it seems that the use of TAM as adjuvant therapy for BC seems more beneficial in postmenopausal patients as the drug minimizes the risk of vascular disease by significantly improving the serum lipid profile.
In summary, our data suggest that plasma TG levels rise during TAM treatment in all APOE genotypes, indicating a need for careful cardiovascular monitoring of BC patients receiving TAM to avoid possible complications. With regard to the menopausal state, significant reductions observed in TC, LDL-C, and LDL-C/HDL-C ratio after TAM therapy point to a more beneficial effect of treatment on the lipid profiles of postmenopausal than premenopausal patients.
Footnotes
Acknowledgements
The authors thank M. Rubio for statistical support and L.M. Chicharro for technical help.
Abbreviations
The study and the procedures followed were in accordance with the ethical standards of the review board of the Hospital de Getafe (Madrid, Spain) and with the Helsinki Declaration.