
Abstract
Background
Prolonged postoperative ileus (PPOI) is a common problem after major abdominal surgery and can cause postoperative morbidity, extended hospitalization, as well as increased health care costs.
Aim
To investigate whether the levels of cytokines from abdominal exudate are predictive for early diagnosis of PPOI after colorectal surgery.
Methods
One hundred patients who had undergone elective resection for carcinoma of the sigmoid or rectum were recruited. The abdominal exudate was obtained from a drain tube after surgery to examine the levels of C-reactive protein (CRP), procalcitonin (PCT), and tumor necrosis factor alpha (TNF-α). The relationship between cytokine levels on postoperative day 1, 3 and 5 and the occurrence of PPOI was analyzed.
Results
Eight patients developed PPOI, which was diagnosed on postoperative day 10-15. PCT levels on postoperative day 1 and 3 were not significantly different between the 8 patients who developed PPOI and the 92 patients without PPOI. In contrast, PCT levels on day 5 were significantly higher in patients who developed PPOI than in patients without PPOI. The levels of CRP and TNF-α were irregular from day 1 to 5, and were not significantly different.
Conclusions
Increased PCT levels in abdominal exudate may predict PPOI in the early period following colorectal surgery.
Keywords
Introduction
Postoperative ileus (POI) is a transient impairment of bowel motility after major surgery (1). After abdominal operations such as colectomy, postoperative bowel recovery takes 3-5 days (2). Patients with prolonged postoperative ileus (PPOI) often have nausea and vomiting, abdominal distension and/or pain, and delayed passage of flatus and stool. PPOI is often associated with prolonged length of hospital stay, readmission, high morbidity and mortality (3). Although PPOI is severe, requiring early diagnosis and immediate treatment (4), the early diagnosis of PPOI remains difficult due to a lack of appropriate laboratory parameters (5). Early detection of PPOI is critical for applying early intervention and minimizing mortality.
Cytokines are critical factors in the systemic inflammatory response syndrome (SIRS) (6). The cytokines procalcitonin (PCT), C-reactive protein (CRP) and tumor necrosis factor alpha (TNF-α) mediate the acute-phase response in humans (6, 7). Peritoneal cytokines can predict early postoperative inflammatory reactions as well as serious surgical complications (8). For instance, monitoring of peritoneal cytokine levels after elective gastrointestinal surgery may indicate severe intraabdominal complications (9). The present study was conducted to understand the potential importance of peritoneal cytokines in early prediction of PPOI following colorectal surgery.
Patients and Methods
Patients
The study recruited 100 consecutive patients (60 men and 40 women) with carcinoma of the sigmoid colon or rectum who were scheduled to undergo elective open anterior resection under general anesthesia between January and December 2011. None of these patients had an ileostomy during the operation. A patient-controlled analgesia (PCA) pump of morphine chlorhydrate was employed for 48 hours, and the dose of morphine chlorhydrate used in the pump was recorded. Exclusion criteria included patients who had undergone preoperative radiotherapy or chemotherapy; patients who had to undergo emergency surgery; and patients who had been administered antiinflammatory drugs such as immunosuppressants or corticosteroids preoperatively for infectious or inflammatory diseases.
The 100 eligible patients were aged 24-87 years (average 59 years) at the time of surgery. The carcinoma sites were the sigmoid colon in 26 patients and the rectum in the remaining 74 patients. Bowel resection with end-to-end anastomosis was performed with the aid of circular staplers. Prior to peritoneum closure, a silastic drainage tube was placed in the base of the pelvis in all patients, which was removed 5-12 days after the operation.
Definition of prolonged postoperative ileus
POI is common 3-5 days after major abdominal surgery. It develops in most patients undergoing abdominal surgery and is considered a normal phenomenon during the postoperative course. However, it was reported that among patients who underwent abdominal operations, 7% of POIs would develop into PPOI with the observed clinical manifestations and radiological imaging for ileus, which usually needs clinical intervention (4, 11). It was found that the recovery of motility and absorption by the small bowel occurs within hours, whereas recovery of gastric and colonic functions may take as long as 2-5 days (10). Based on the above observations, POI lasting longer than 6 days after surgery and with evident clinical symptoms and radiological imaging which should be diagnosed at an early stage for earlier treatment is a better clinical definition of PPOI (11) and was adopted in our study. The enrolled patients were divided into 2 groups: a PPOI group (with clinical symptoms and radiological imaging of PPOI) and a No-PPOI group (without clinical symptoms and radiological imaging of PPOI).
Sampling
Samples of abdominal exudate were collected from the abdominal drains on day 1, 3 and 5 after the operation. All samples were obtained within 2 hours of drainage bag emptying in the morning. Five milliliters of abdominal exudate was centrifuged at 5000 rpm for 15 minutes before being stored at −80°C.
The levels of PCT, CRP and TNF-α were measured by ELISA (Ray BioR Human PCT, CRP and TNF-α ELISA Kit protocol, Shenggong, Shanghai, China). The procedure was performed as described in the kit.
Data and statistical analysis
The SPSS software version 13.0 was used for statistical analysis. Normally distributed data were expressed as mean ± standard deviation while abnormally distributed data were expressed as median (range). The changes in PCT, CRP and TNF-α levels were analyzed by repeated-measures analysis in a general linear model, after the logarithmic transformation of raw data into normally distributed data. The qualitative data were compared with Fisher's exact test or the chi-square test. P<0.05 was considered statistically significant.
Results
Clinical characteristics
Clinically proven PPOI occurred in 8 of the 100 patients (8.0%) (6 men and 2 women). The median day of the PPOI diagnosis was day 12 (range 10-15) after the operation. Of the 8 PPOI patients, 6 were given conservative treatment to promote bowel movements and the other 2 patients were urgently reoperated on for adhesiolysis. All 8 PPOI patients recovered well after treatment. There was no mortality in this study. As shown in Table I, the clinical variables including age, sex, BMI, location of carcinoma, intraoperative blood loss, operative time, dose of morphine during PCA and days of postoperative hospital stay were well balanced between the 2 groups, except that the time to first passage of flatus was longer in the PPOI group than the No-PPOI group.
Data Of Patients Undergoing Anterior Resection Of The Sigmoid Or Rectum
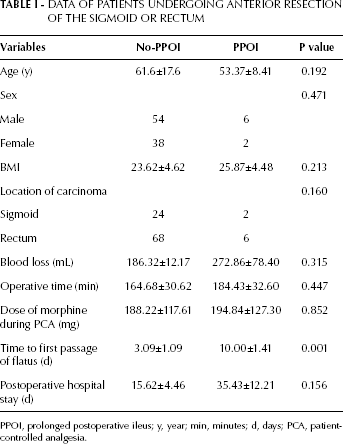
PPOI, prolonged postoperative ileus; y, year; min, minutes; d, days; PCA, patient-controlled analgesia.
Peritoneal cytokines
The values and changes of PCT, CRP and TNF-α levels on postoperative day 1, 3 and 5 between the 2 groups are shown in Figure 1. Repeated-measures analysis revealed that the changes in PCT levels were significantly different between the 2 groups. Tables II-IV show the levels of PCT, CRP and TNF-α on postoperative days 1, 3 and 5, respectively. There was no significant difference in PCT levels on postoperative days 1 and 3 between the 8 patients who developed PPOI and the 92 patients without PPOI. However, the level of PCT on day 5 was significantly higher in the PPOI group than in the No-PPOI group. The CRP level increased from day 1 to day 3 and decreased on day 5 in both groups. The level fluctuated markedly but nonsignificantly. Finally, the TNF-α level increased from day 1 to day 3 and decreased on day 5 in patients who developed PPOI. In the No-PPOI group the TNF-α level decreased from day 1 to day 3, and changed nonsignificantly from day 3 to day 5. Similar to CRP, the TNF-α level fluctuated markedly but nonsignificantly.
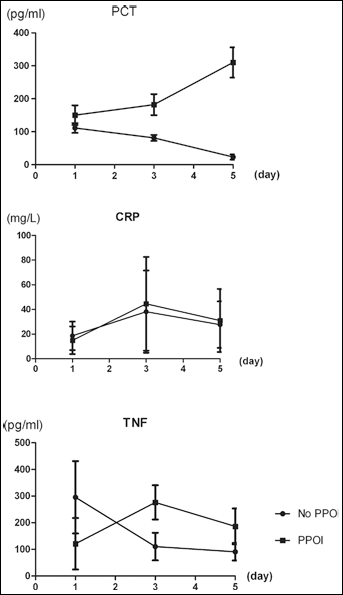
Changes (mean±SD) in PCT, CRP and TNF-α levels on postoperative days 1, 3 and 5. PPOI, prolonged postoperative ileus.
Peritoneal Pct Levels On Postoperative Day 1, 3 And 5 (Pg/Ml)
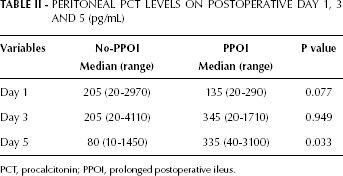
PCT, procalcitonin; PPOI, prolonged postoperative ileus.
Peritoneal Crp Levels on Postoperative Day 1, 3 AND 5 (mg/L)
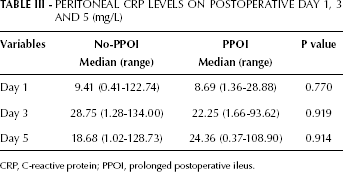
CRP, C-reactive protein; PPOI, prolonged postoperative ileus.
Peritoneal Tnf-α Levels on Postoperative Day 1, 3 AND 5 (pg/mL)
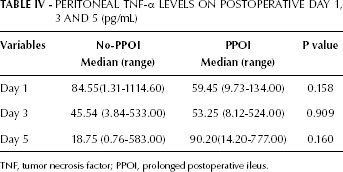
TNF, tumor necrosis factor; PPOI, prolonged postoperative ileus.
Discussion
Acute bowel obstruction leads to high morbidity, increased hospitalization costs and emergency conversion surgery (11, 12). The traditional diagnosis relies on clinical signs including hypotension, leukocytosis, constant pain, fever, tachycardia, base deficit, peritoneal signs, as well as metabolic acidosis (13). Abdominal CT scan can also be employed in the diagnostic workup (14). Early and accurate treatment is critical for the safety of the patients. However, there it is still a lack of sensitive diagnostic biomarkers (15) and few reliable parameters have been developed (16). The present study evaluated the predictive value of peritoneal cytokines for the early diagnosis of bowel obstruction following surgery for colorectal carcinoma. Although the potential value of plasma cytokines for the diagnosis of PPOI has been assessed before (17), cytokines from abdominal exudate have not been examined. Our study is the first to examine the relation between peritoneal cytokine changes and ileus in the postoperative period.
Peritoneal cytokines were found to increase significantly after abdominal surgery and have therefore been correlated with postoperative complications (9). We measured the cytokines PCT, CRP and TNF-α on postoperative days 1, 3 and 5 to examine their relation to PPOI development. In normal conditions, peritoneal cytokines peaked on the first postoperative day and decreased thereafter (18). Abnormal upregulation of peritoneal cytokines in the first 5 days therefore may predict the appearance of intraabdominal ileus.
PCT is a very expedient inflammatory marker (19). It is a 116-amino acid prohormone of calcitonin and is produced in the medullary C cells of the thyroid. The basal PCT levels in serum are low (<0.05 ng/mL) (20) but will increase after infection. Peritoneal mesothelial cells, leukocytes and fibroblasts are involved in this upregulation (21). Release of PCT can be triggered by microbial antigens such as endotoxins, or indirectly by the immune response (17). PCT has been considered as one of the acute-phase proteins after severe systemic bacterial infection (13). Castelli et al (22) reported that PCT was a more useful parameter than CRP, allowing faster and more valid prediction of infectious complications. In addition, Soybel and Zinner (23) found that ileus is correlated with increased local inflammation responses and immune cell infiltration, as was proved in other studies as well (24). PCT presents as a mediator reflecting intestinal irritation as well as a pathogenetic factor involved in secondary attenuated gastrointestinal motility (25).
Many pathogenetic mechanisms have been proposed to account for the impaired gastric electrical activity during ileus. We suppose that the local inflammatory status may play an important modulating role. The association of ileus with increased systemic levels of the proinflammatory cytokines PCT and CRP was documented in our study. As other authors reported, this systemic reaction was activated on a local level and a local inflammatory milieu initiated a systemic cytokine network (26). Previous studies (23) revealed that the normally resident macrophages within the muscularis are rapidly activated during impaired intestinal motility, thus initiating an inflammatory cascade of events including the upregulation of chemokines, cytokines and kinetically active substances (27). This local inflammatory status leads to the extravasation of leukocytes to the circular muscle layer. In conjunction with increased adhesion molecule expression, leukocytes course through the muscularis externa, eventually inhibiting gastrointestinal smooth muscle contractility.
The level of PCT has been proposed as a prognostic factor since 1992 (28), and has been applied as such in several conditions including sepsis, acute pancreatitis, infectious and noninfectious SIRS as well as other postoperative complications (29). Peritoneal cytokines were chosen to measure the postoperative inflammatory reaction in major abdominal surgery because of their better sensitivity compared with systemic cytokines (8). In our subsequent studies, measurements of systemic and peritoneal PCT before and after surgery will be carried out and evaluated. We will ascertain whether the PCT level in peritoneal fluid will be affected by the systemic circulation. Furthermore, we will compare the systemic and peritoneal PCT levels after surgery to indicate which is the more sensitive in predicting PPOI.
In conclusion, the measurement of PCT levels from abdominal exudate may lead to an early diagnosis of PPOI after colorectal surgery. In addition, consecutive PCT examinations would help in the decision to resort to emergency surgery or continuation of non-operative management in clinical practice.