
Abstract
Background:
Aerosol delivery in-line with high-flow nasal cannula (HFNC) has been increasingly utilized. However, most of the studies were conducted using models with mouth closed, which might not reflect the real-life scenario. Thus, we aimed to compare different simulated models, varying mouth status, and with/without exhaled humidity to explore factors influencing the inhaled dose.
Methods:
A 3D-printed adult nose-mouth-throat (NMT) model was compared with an adult training manikin for intubation. A collecting filter was connected between the trachea and breath simulator, set to adult breathing parameters of tidal volume [VT] 470 mL, frequency 21 breaths/min, and inspiratory time [TI] 1.1 s. The mouth was sealed with tape to simulate closed-mouth breathing and removed for open-mouth breathing. A humidifier was placed between the collecting filter and the model lung to simulate exhaled humidity. Albuterol (2.5 mg/3 mL) was delivered via a vibrating mesh nebulizer (VMN) positioned at the humidifier’s outlet in the HFNC device (Airvo2), with flows set at 15 L/min and 45 L/min. Each experiment was repeated 5 times. The drug was eluted from the collection filter after each run and assayed with ultraviolet spectrophotometry (276 nm).
Results:
The NMT model had higher inhaled dose than the adult manikin in all settings (all P < .05), except for the open mouth-breathing at 15 L/min (21.1 ± 0.6 vs 24.4 ± 1.3, P = .001) (Table 1). At 45 L/min, there was no significant difference between open-mouth breathing and closed-mouth breathing in both models. However, at 15 L/min, closed-mouth breathing of NMT model had a higher inhaled dose than open-mouth breathing (24.7 ± 0.4 vs 21.1 ± 0.6, P = .008), while in the adult manikin, closed-mouth breathing had a lower inhaled dose than open-mouth breathing (18.9 ± 1.4 vs 24.4 ± 1.3%, P = .008). In the adult manikin during open-mouth breathing, the inhaled dose with exhaled humidity was higher than without exhaled humidity in both flow settings (all P < .05) (Figure 1).
Conclusions:
Trans-nasal pulmonary aerosol delivery can be affected by simulating model, mouth status, and exhaled humidity.
Results of aerosol delivery via HFNC with different models and mouth status
Mouth status
Flow setting(L/min)
Inhaled dose with 2 model, %
P
NMT model
Adult manikin
Closed
15
24.7 ± 0.4
18.9 ± 1.4
<0.001
45
6.5 ± 0.9
5.2 ± 0.8
0.038
Open
15
21.1 ± 0.6
24.4 ± 1.3
0.001
45
7.7 ± 1.0
6.1 ± 0.5
0.013
P
15
0.0079
0.0079
45
0.087
0.0952
Figure 1. Aerosol delivery via high-flow nasal cannula with versus without exhaled humidity in adult manikin.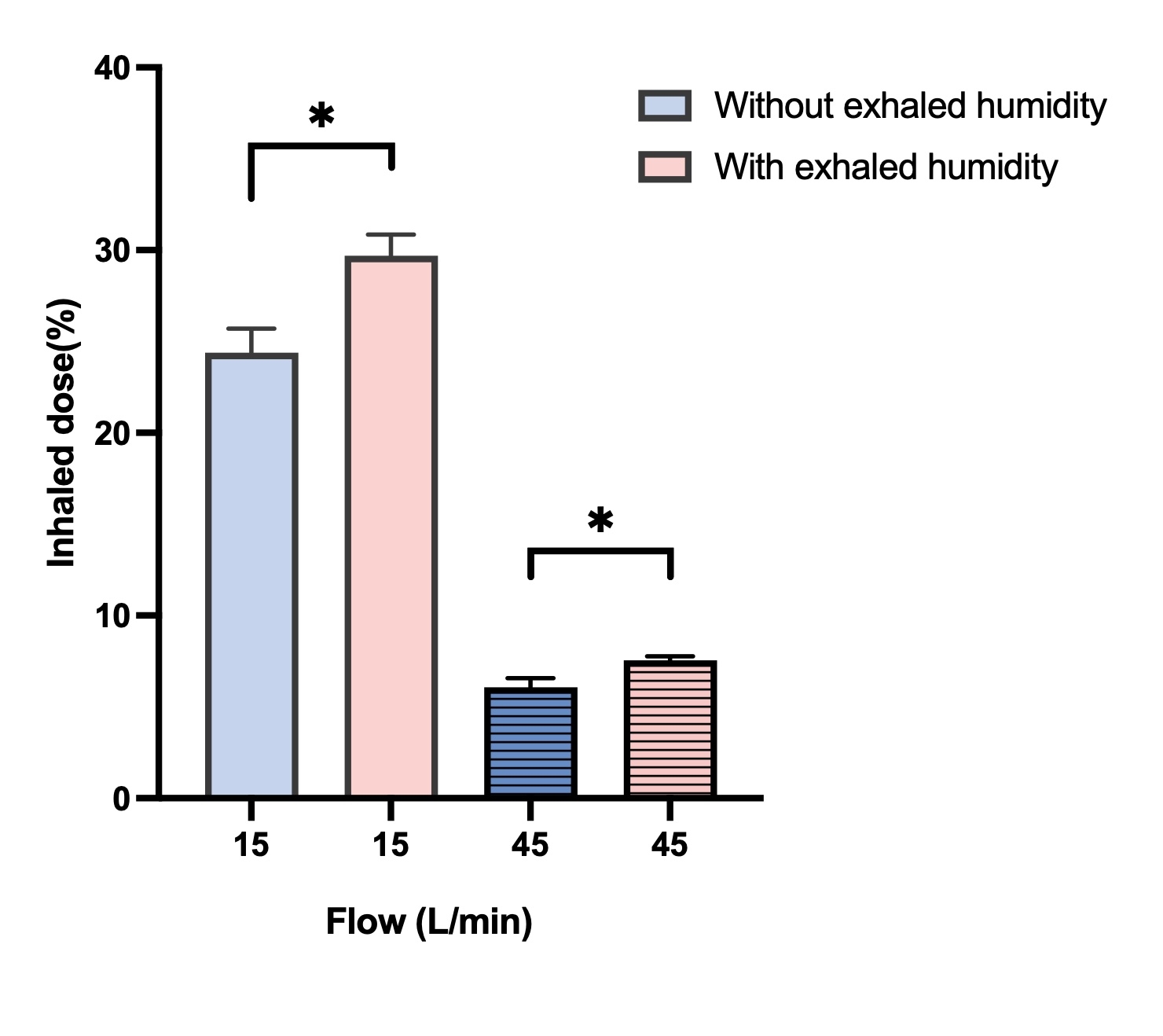
Get full access to this article
View all access options for this article.