
Abstract
Background:
Successful spontaneous breathing trials (SBT) have been recognized as a measure of extubation readiness in PICUs. In ongoing quality improvement (QI) projects at our institution we have focused on decreasing time from a successful SBT to extubation and have identified multifactorial reasons for delays. Often, reasons for these delays in extubation are non-respiratory related issues such as nursing and provider orders, including NPO status and sedation plan. We aimed to examine the effectiveness of instituting a multidisciplinary extubation huddle to discuss extubation readiness in detail after 30 min of a successful SBT on the time to extubation at our institution’s PICU (260-bed pediatric hospital, Level 1 Trauma, Level IV NICU, 24 PICU beds).
Methods:
An IRB-approved retrospective data review was completed which included PICU data from 1/1/2022–12/31/2023. Education for the extubation huddle occurred in December of 2022 with implementation clinically 1/1/2023 thus, 2022 was considered the pre-implementation period and 2023 the post-implementation period. Data analysis included the mean time from first passed SBT to extubation in hours, endotracheal tube days, and adherence to the new extubation huddle process. Intubated PICU patients who did not qualify for an SBT were excluded from analysis.
Results:
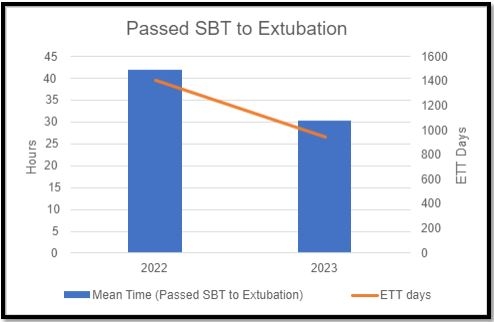
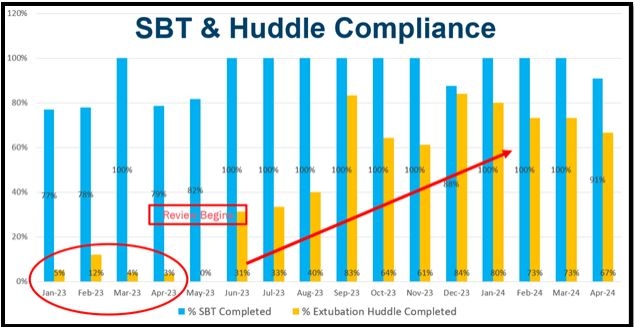
In 2022, pre-intervention, the mean time to extubation from first passed SBT was 41.98 h and decreased to 30.19 h in 2023, post-intervention (Figure 1). Adherence was slow to increase with first quarter 2023 having 7% adherence with the process, but fourth quarter, after increasing education, adherence was 70%. Overall endotracheal tube days decreased from 1,408 in 2022 to 947 in 2023.
Conclusions:
In our single PICU, institution of a standardized multidisciplinary extubation huddle resulted in a reduction in mean time from first passed SBT to extubation. The huddle was feasible, but required education to improve adherence over time. Many intervening factors play into the decision to extubate, thus making isolation of the huddle effect challenging. More research and QI is warranted to optimize time to extubation as well as the effect of extubation huddles.
Get full access to this article
View all access options for this article.