
Abstract
Background:
Pediatric sleep medicine is a complex field that requires a multi-disciplinary clinical team to support operations. Our pediatric sleep labs provide services for 1,800 patients annually in 3 states. Due to the complex nature of polysomnography testing, there is value in having a clinical team member scheduling sleep studies in the pediatric population. A specialty nurse in this role vacated the position, allowing the team to reevaluate the possibility of filling the role with an RPSGT or RT. We aimed to review the cost implications of using an RPSGT or RT instead of a specialty RN for this role and the impact on operational patient outcomes.
Methods:
In an IRB-exempt retrospective review, a cost analysis and operational metrics review were performed to compare the cost savings related to changing the role from specialty RN to RPSGT/RT. Additionally, associated patient operational outcomes (no-show, cancel, early terminations, patient emergencies, # of studies performed) from 11/1/2023-4/30/2024 were reviewed to determine the operational patient impact in a 3-month period with a specialty RN and a 3-month period with an RT/RPSGT in the scheduling position. An extensive job description overview was performed, and the role was posted upon approval from 12/19/2023 to 1/29/2024. Formal interviews were conducted for candidate selection.
Results:
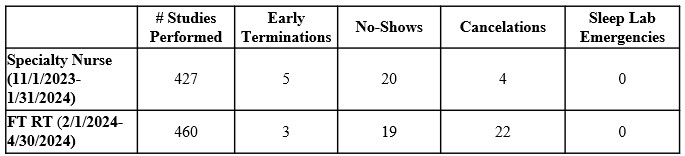
Salary and benefit cost savings ranging from $57K to $79K annually were present when transitioning this role from a specialty RN to an RPSGT or RT (Figure 1). Candidates from both fields expressed interest in the role, which was offered and accepted by an RT on 2/1/2024. There were no significant adverse changes in the number of scheduled studies, early terminations, no-shows, or sleep lab emergencies (n = 0), regardless of scheduler credentials (Figure 2). There was an increase in cancelations likely driven by an insurance process change requiring prior authorization prior to the study implemented by a high-volume payor in January of 2024.
Conclusions:
Transitioning a specialty RN role to RT/RPSGT can save labor costs while providing non-traditional opportunities for sleep and respiratory professionals within their scope of practice. In some facilities, costs may increase if scheduling is transitioned from central scheduling to a clinician. Further studies must be done to evaluate the impact on patients and caregivers when a clinical caregiver is available during the scheduling process regarding successful study preparation, expectations, and completion.
Figure 1 details the cost analysis based on credential type. Figure 2 details the operational metrics that may be impacted by a sleep scheduler in a 3-month period with an RN scheduler and a 3-month period with an RT scheduler.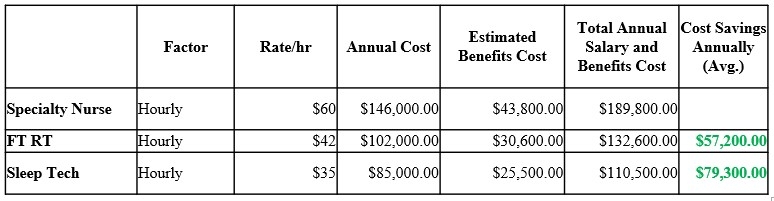
Get full access to this article
View all access options for this article.