
Abstract
Background:
Bronchiolitis management of pediatric, critically ill patients can be challenging and resource intensive. Implementing AAP based guidelines and developing collaborative education is essential for best practice care. High-flow nasal cannula (HFNC) protocols are necessary to identify and treat patients efficiently and may prevent unwarranted ICU transfers. This was a quality improvement project implementing HFNC management on pediatric wards as a strategy to decrease ICU transfers.
Methods:
Previous pediatric floor HFNC L/min limits did not allow continuation of care within pediatric ward, requiring patients needing HFNC an ICU transfer. In 2023, bronchiolitis protocol was developed and presented to collaborative practice team. New guidelines increased L/min flow in correlation to specific weight and age in reflection of maintaining frequent care. Primary outcome was to monitor ICU days prevented when maintaining patients on wards, avoiding ICU transfer after new protocol implementation. Secondary outcomes were to decrease length of stay (LOS) while improving practice. Institutional Review Board committee approved for monitoring purposes.
Results:
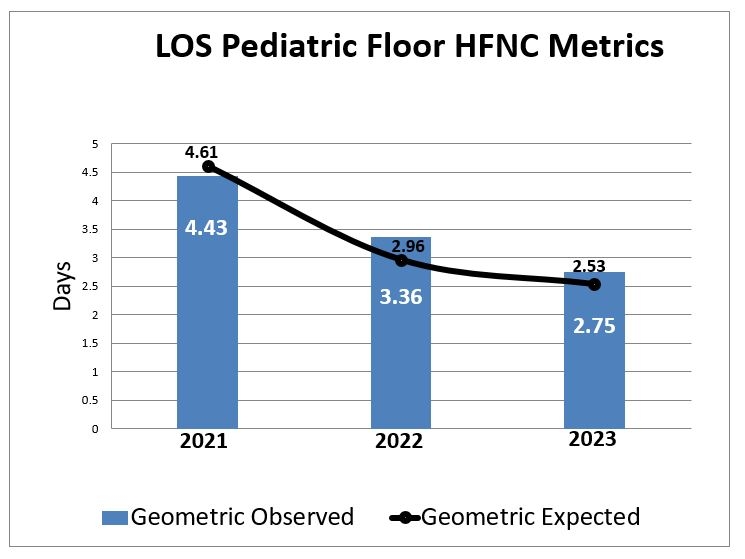
Pre-protocol, 79 HFNC patients transferred from pediatric floor to ICU in 2021 and subsequently 68 in 2022. Post-protocol, 128 patients in 2023 were above old HFNC policy that met new criteria. Of patients, 36 (28%) HFNC patients were transferred to ICU, with 69.4% of transfers due to increased respiratory distress, 11.1% surgery consults, and 19.4% required extensive bronchodilator intervention. New HFNC policy resulted in 53% reduction of internal transfers. Total of 92 patients were discharged from pediatric floor that would have met previous ICU criteria with 215 ICU days prevented. Pre-protocol, HFNC metric observed LOS for 2021 was 4.43 d and 3.36 d in 2022. Post-protocol in 2023, LOS decreased to 2.75 d. Cost difference between average PICU patient day and pediatric floor day is $663, with annual cost saving calculated as $142,600.
Conclusions:
Implementing an evidence-based practice and promoting efficient HFNC management decreased hospital LOS and ICU transfers. Change in management allowed the ICU to keep open beds for patients of higher acuity and maintain community access. Designing safe processes and conducting education made a direct impact to valued respiratory care. Reducing LOS improved operational, financial, and clinical outcomes by decreasing cost of patient care with more efficient bed management flow.
New Pediatric Floor HFNC Limit
Age
Maximum Flow
1 day - 1 year
1L/kg up to 10L
1 - 5 years
1L/kg up to 12L
>5 years
14L
Get full access to this article
View all access options for this article.