
Abstract
Background:
Children with ≥2 ED visits or ≥1 hospitalization for asthma are considered high risk. There is a strong link to asthma morbidity, social determinants, and neighborhood conditions. The Child Opportunity Index (COI) is a publicly available resource for measuring neighborhood conditions where higher scores reflect higher opportunity. Children living in neighborhoods with a very low or low score are at higher risk for asthma morbidity and may benefit from care coordination and health navigation to address barriers affecting health outcomes.
Methods:
Starting July 1, 2023, children (<6 years) who are seen in our children’s hospital primary care and pulmonary clinics for asthma were identified for the asthma intensive reinforcement (AIR) QI pilot via EMR if they had ≥ 2 ED visits and/or ≥1 hospitalizations in the preceding 12 months and lived in identified zip code with a low or very low COI score. Children > 6 years of age and/or who were already enrolled in a home visit program, currently being managed within our multidisciplinary asthma clinic, or their primary pulmonary provider requested that they not be included in the AIR pilot were excluded. The multidisciplinary AIR team reviewed the EMR monthly for each child to determine if there were any clinical (communication, refill, access) or social barriers potentially preventing the child from following their asthma action plan. Over a 6-month period an identified team member would call the child’s caregiver to review the AAP, identify and/or address any barriers to care. Identified clinical and/or social barriers and health care utilization was tracked prior and after the start of the AIR pilot.
Results:
A total of 17 children were initially identified, 8 were excluded. The demographics were median age 4 y, male (78%), English (56%), Black (44%) and Hispanic (56%). There was difficulty contacting 33% of the caregivers. Findings included 33% had social barriers (food, transportation, financial insecurity), 66% had at least one clinical barrier, and 22% had a subsequent hospitalization or ED visit within 6 months.
Conclusions:
Clinical and social barriers can negatively impact children with asthma being able to follow their asthma action plan. Addressing these barriers after a hospitalization or clinic visit through ongoing care coordination and health navigation can decrease health care utilization. Factors affecting ongoing healthcare utilization may include lack of insurance, beliefs, and ongoing exposure to environmental triggers.
Asthma Intensive Reinforcement Pilot Demographics
n=9
Median Age
4 yrs (SD 1.13)
Gender
Male
78% (n=7)
Female
22% (n=2)
Language
English
56% (n=5)
Spanish
22% (n=2)
Other (French, Amharic)
22% (n=2)
Race
Black/African American
44% (n=4)
White
34% (n=3)
Other
22% (n=2)
Ethnicity
Hispanic
56% (n=5)
Not Hispanic
44% (n=4)
Follow-Up
Difficult to contact
34% (n=3)
Social barriers
34% (n=3)
Clinical barriers
66% (n=6)
Healthcare utilization
22% (n=2)
:Local Child Opportunity Index 2.0 Neighborhood Mapping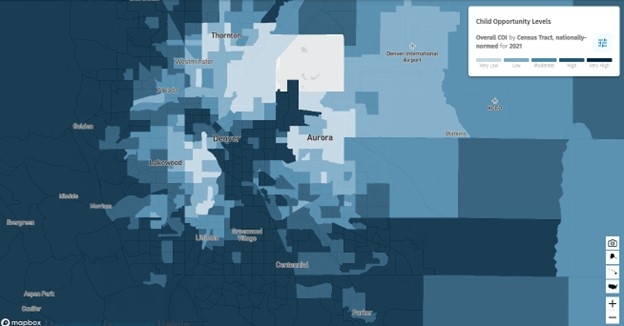
Get full access to this article
View all access options for this article.