
Abstract
Background:
Accidental decannulation (AD) of a tracheostomy tube is an unfortunate complication with the potential for dire consequences. With the goal of developing a quality improvement initiative to reduce the cases of AD at our facility, we set out to investigate whether specific variables were more prevalent in past incidents.
Methods:
A retrospective analysis was performed spanning the course of 16 months at Brigham and Women’s Hospital in Boston. Patient, system, and airway related data was collected by means of chart review and internal incident reports and was exclusive to the adult population. This study was approved by the BWH Human Research Affairs Committee.
Results:
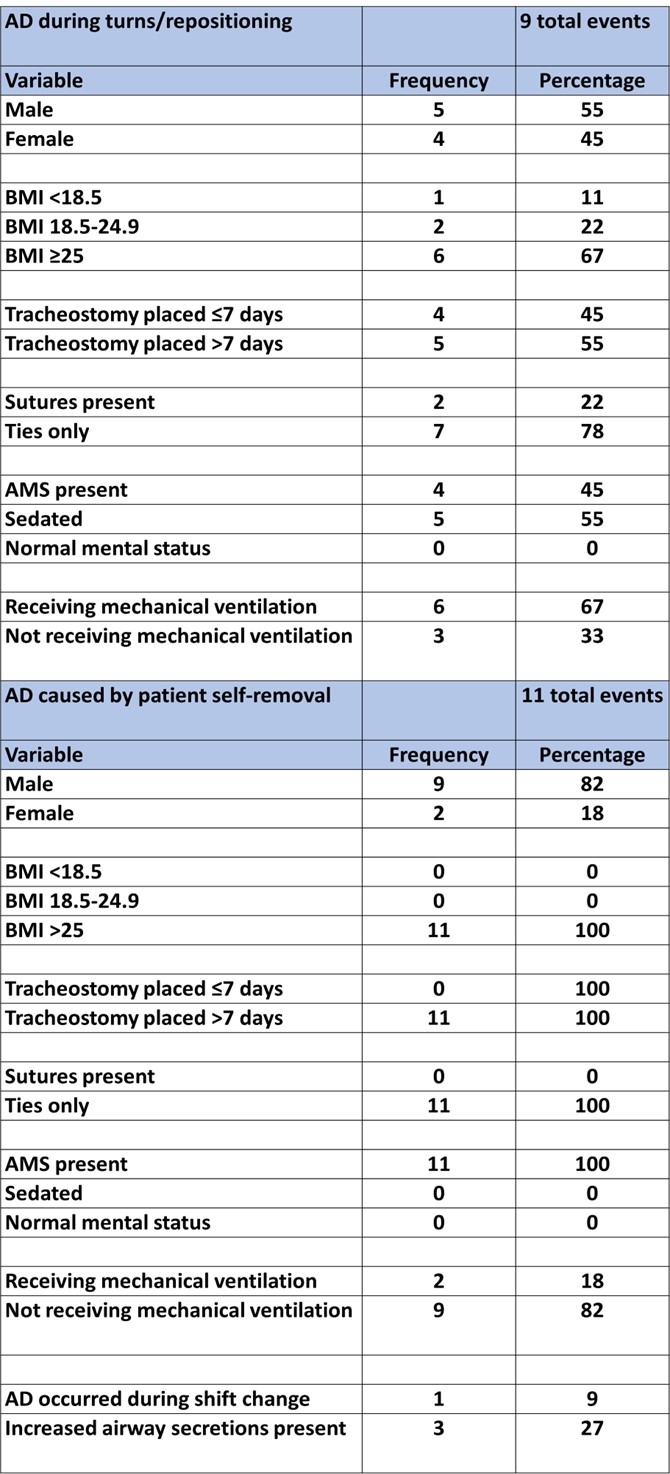
During the 16 months reviewed, there were 28 events of AD. 61% were male, 39% were female. 82% of the patients that experienced AD were classified as either overweight or obese. The most common age demographic revealed 71% were age 60 or older. 14% had a tracheostomy tube placed in ≤ 7 d, 86% had a tracheostomy tube placed in > 7 d. 93% of tracheostomy tubes were secured with ties only, 7% were secured with ties and sutures. A timeline of events revealed that 57% of all ADs occurred during the middle of the shift for both day and night shift, represented by the hours of 11:00-15:00 and 23:00-03:00. Only one event occurred during shift change. The two most common causes of AD involved patient repositioning/turns (32%) and patient self-removal (39%). Of the patients who self-decannulated, 100% exhibited altered mental status (AMS) with variable degrees of delirium, were classified as overweight or obese, had a tracheostomy tube placed >7 d, and had tracheostomy tubes secured with ties only. 82% of events occurred in a non-ICU setting, 82% of patients were not on mechanical ventilators, and 82% were male. ADs that occurred during turns/repositioning revealed 78% occurred in the ICU, 67% of patients were classified as overweight or obese, 78% of tracheostomy tubes were secured with ties only, and 67% were receiving mechanical ventilation.
Conclusions:
The analysis of past AD events provided valuable information towards narrowing our areas of focus in creating our initiative. We were able to identify the need to address best practices for patient repositioning to avoid AD. The need for improvement to prevent AD in patients exhibiting AMS was made apparent. Focus was also directed towards investigating the prevalence of events occurring during the middle of standard shifts.
Table 1: Patient demographic, airway, and system data Table 2: AD resulting from turns/repositioning and self-removal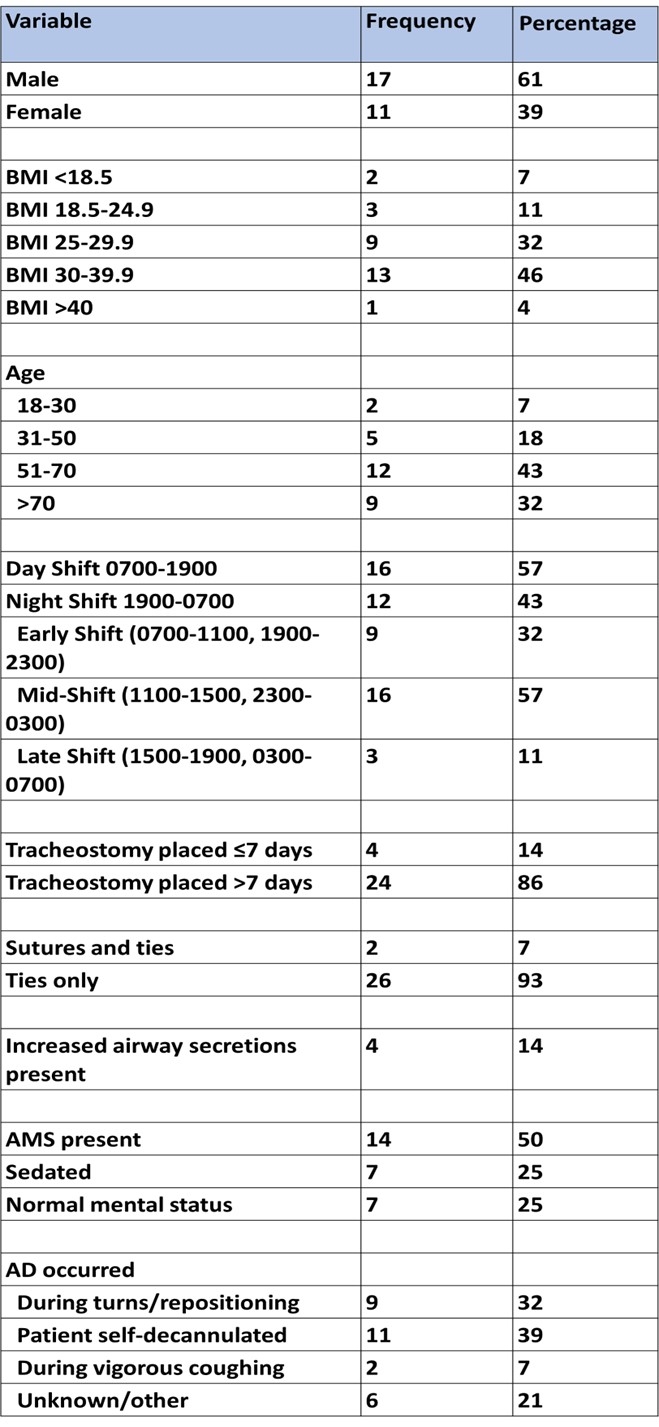
Get full access to this article
View all access options for this article.