
Abstract
Background:
Inhaled nitric oxide (iNO) is frequently delivered with noninvasive methods at our institution for children with congenital heart disease. This includes a high-flow nasal cannula (HFNC) system and noninvasive ventilation (NIV). Previous evaluation of iNO delivery via HFNC in an infant model found that delivery efficiency ranged from 63-78% (Berlinski A, Moore M, Willis D. Inhaled nitric oxide delivery in a 7-month-old spontaneously breathing infant model. J Cystic Fibrosis 2023;22(Suppl):S6). The aim of this study was to evaluate iNO delivery with NIV and to compare it to previously obtained data using HFNC system.
Methods:
An anatomically correct 3D airway model of a 7 month-old child was connected in series to a scavenger filter and breathing simulator (frequency 30 breaths/min, VT 50 mL, I:E 1:2). A nasal cannula (Medium Optiflow Jr 2, Fisher & Paykel) was used with flows 2, 6, and 10 L/min for the HFNC system. NIV was used with a nasal cannula (RAM, Neotech) and ventilator (Servo-i, Getinge) with breathing frequency 30 breaths/min, pressure control 10 cm H2O, and PEEP 8 cm H2O. The iNO system (INOMax, Mallinckrodt) was set to deliver 5, 20, and 40 ppm. NO analyzers were placed before the nasal cannula and at the tracheal level. Delivered and tracheal iNO measurements were recorded after 3 min and experiments were performed in quadruplicate. Ambient NO and NO2 were monitored. Tracheal iNO/dialed iNO(%) values were calculated. ANOVA for repeated measures followed by Tukey for multiple comparisons was used to compare NIV data (different iNO concentrations). Unpaired t-test was used to compare NIV and HFNC data at each iNO concentration. A P < .05 was considered statistically significant.
Results:
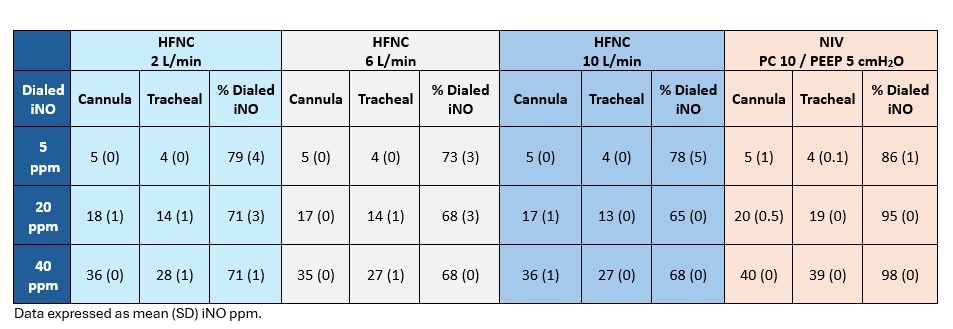
NIV system delivery efficiency ranged from 86-98% and increased with increasing iNO concentration. Tracheal percentage was higher for 5, 20, and 40 ppm with NIV than HFNC at 2 L/min (P < .04), 6 L/min (P < .001), and 10 L/min (P < .001). Ambient NO and NO2 were 0 for all experiments.
Conclusions:
Delivery of iNO with a NIV system was very efficient. Practitioners should be aware that when transitioning to ventilatory support with HFNC a decrease in iNO delivery efficiency may occur.
Experimental Set-up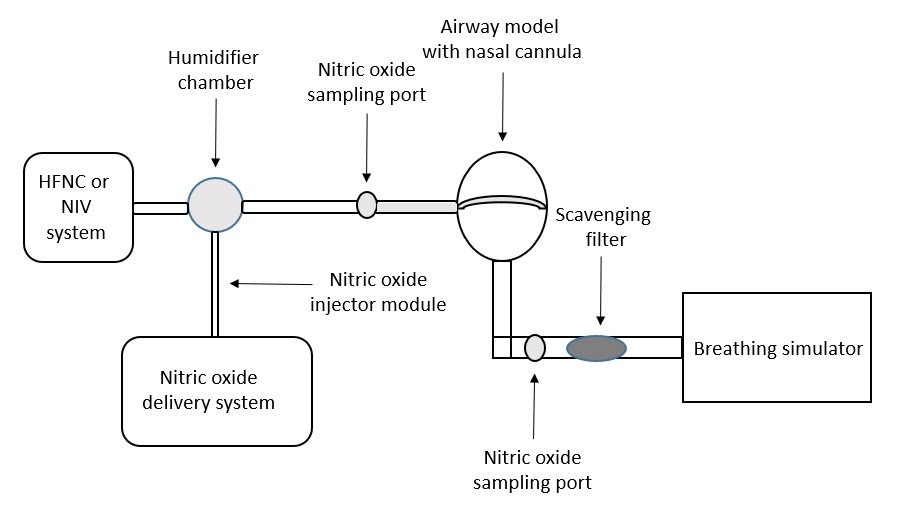
Get full access to this article
View all access options for this article.