
Abstract
Background:
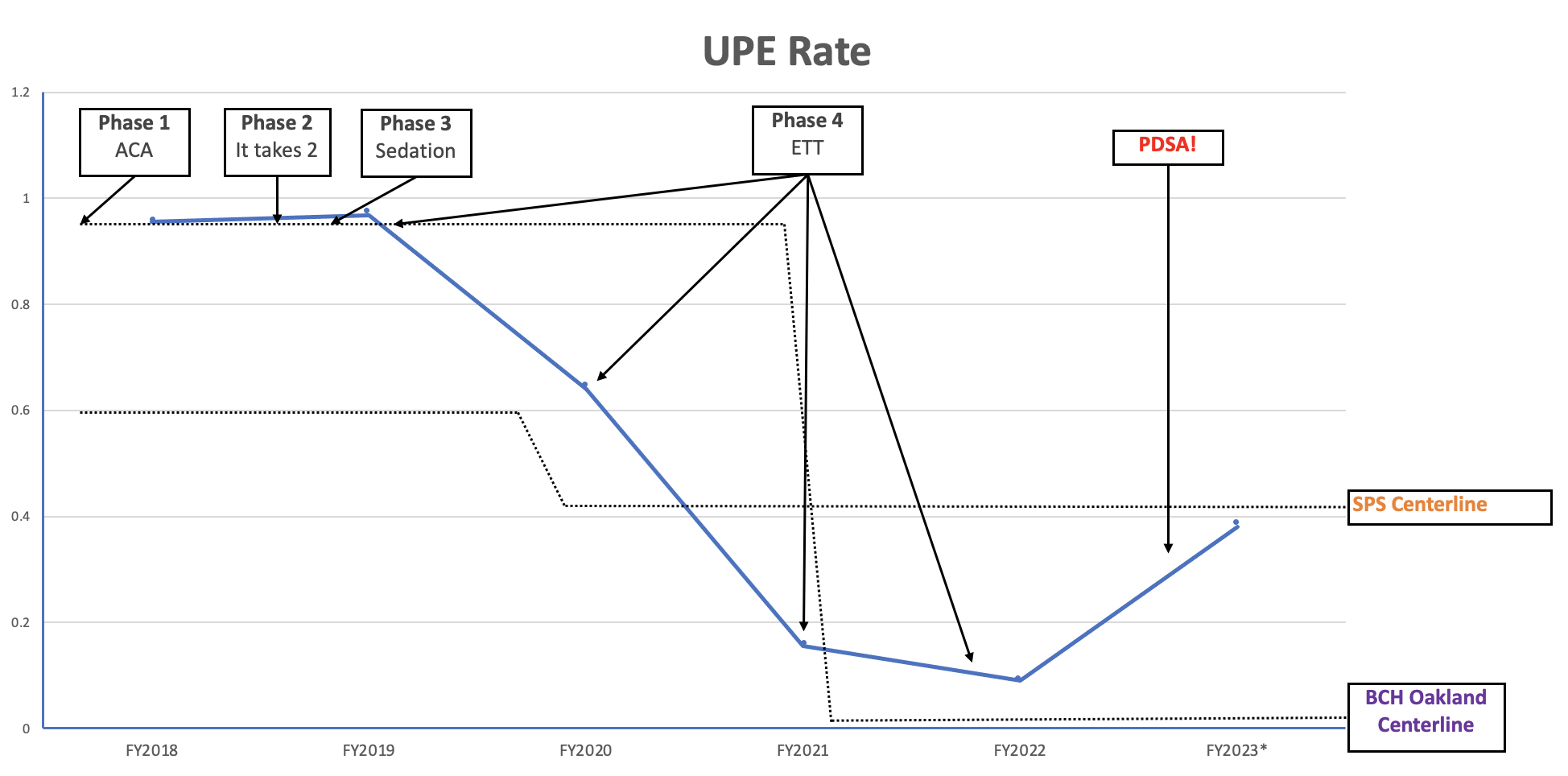
Unplanned extubations (UPEs) in the PICU can result in increased mortality, morbidity, and length of stay. Our rates (events per 100 patient ventilator days) were consistently above the benchmark from the Solutions for Patient Safety (SPS) national collaborative, and were on track to increase even further in early 2018. We aimed to reduce our annual UPE rate from FY 2018 baseline of 0.96 by 20% per year until we achieved an annual rate below the SPScenterline (0.59 at project initiation).
Methods:
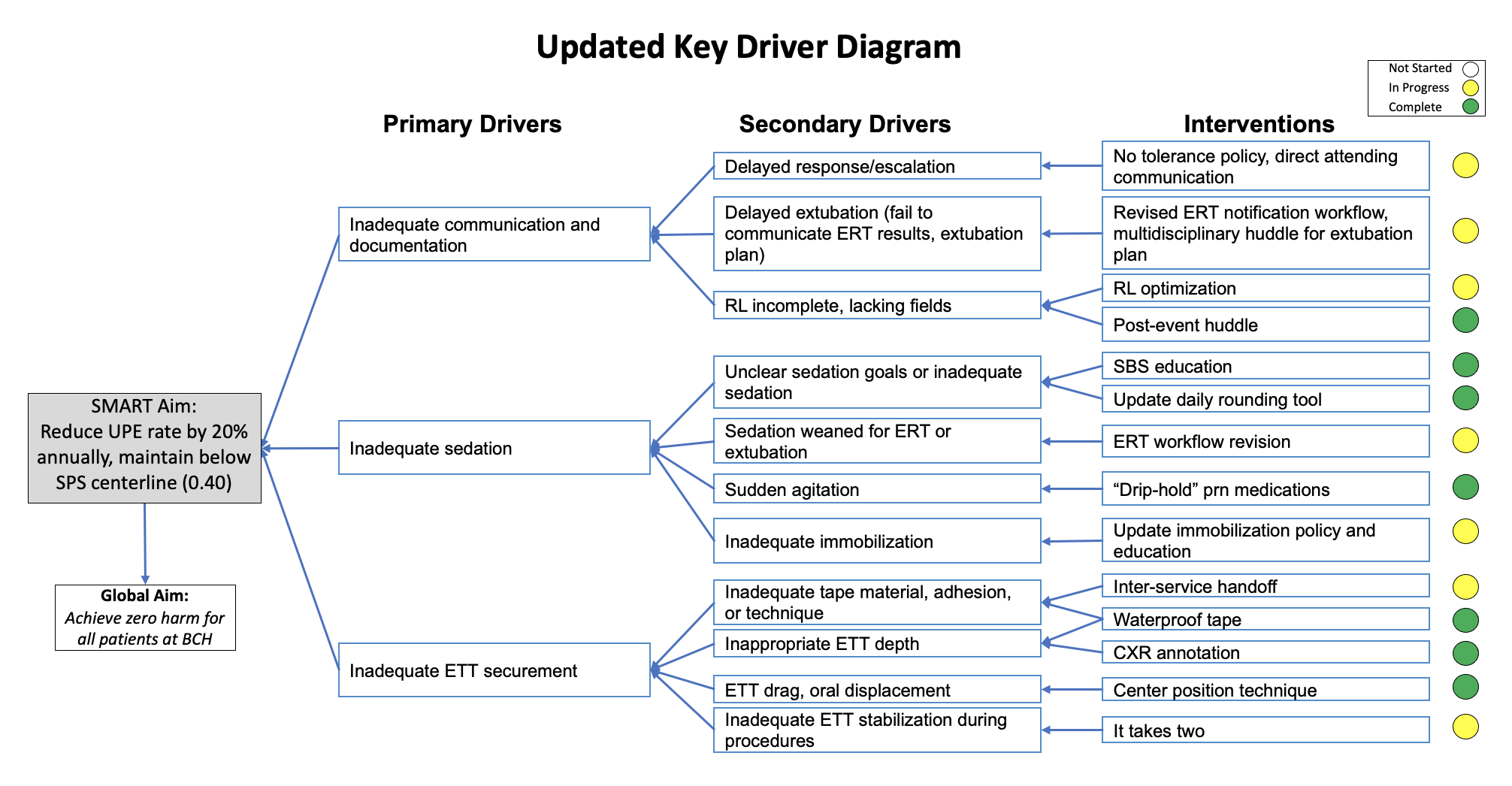
We reviewed 2 years of data, identified root causes, which included inadequate sedation or decreased sedation in anticipation of extubation, sudden agitation (spontaneous or with procedure), movement during procedures, improper tube securement or delayed retaping, inadequate medical immobilization, or excessive secretions. We quantified how often each root cause was the primary cause of an UPE and how often they contributed to an UPE to aid in prioritizing interventions. In planning interventions, we incorporated suggestions from our NICU colleagues who participated in the SPS Unplanned Extubation Pioneer Cohort, including their It Takes Two methodology for securing, repositioning, and/or manipulating endotracheal tubes. Interventions fell into three broad categories: (1) communication/documentation (eg, new procedures and education on escalating concerns, new post-event huddle, and updated event reporting), (2) inadequate sedation (eg, education and discussion around sedation goals, and updated rounding tool), and (3) inadequate endotracheal tube securement (eg, new product trials and adoption of a novel center upper lip taping procedure for children too small for a commercial securement device).
Results:
Compared with our preintervention baseline rate in FY2018, we reduced our average annual rate of unplanned extubations by over 50%, exceeding our goal and the national SPS benchmark.
Conclusions:
A multidisciplinary team using continuous quality improvement can dramatically reduce UPEs in a PICU. Keys to success included collaboration within our interprofessional team, synergy across units/sister institutions and other initiatives (eg, delirium reduction, early mobility), and learning through multicenter collaboratives. Ongoing barriers to sustainability include human resource issues (ie, turnover, burnout, evolving unit culture, ineffective communication among team members and other services, and lack of resources to support ongoing education and auditing), data acquisition, and EMR optimization.
Get full access to this article
View all access options for this article.