
Abstract
Background:
Respiratory therapists in this Tennessee Hospital assisted with administration of influenza vaccines as an added resource to hospital’s employee health department. This expedited meeting the CMS mandate to get 90% of employees vaccinated for influenza. The RTs attended class on the vaccination procedure and documentation of process. RTs were available 24 hours per day and were able to reach evening/night and weekend workers. The RTs would educate on the significance of vaccine to assist in the prevention of influenza. This became a well-respected practice by employees and physicians. In 2015, with Prevnar 13, the RTs were asked by nursing administration to take on the administration/screening of influenza and pneumonia vaccines for hospital patients. This was due to nursing shortage and the required education over a short time frame that would be required for nurses how to screen for the proper vaccines and meet mandated documentation requirement in TN. Since the RTs had been successful with the influenza vaccines, this was a logical step.
Methods:
RTs received daily list of newly admitted patients to screen/administer influenza and pneumonia vaccines and to complete documentation. The RTs spent time educating the patient on vaccines with disease prevention and education of the disease. Influenza and pneumonia are respiratory diseases, so RTs were the perfect choice.
Results:
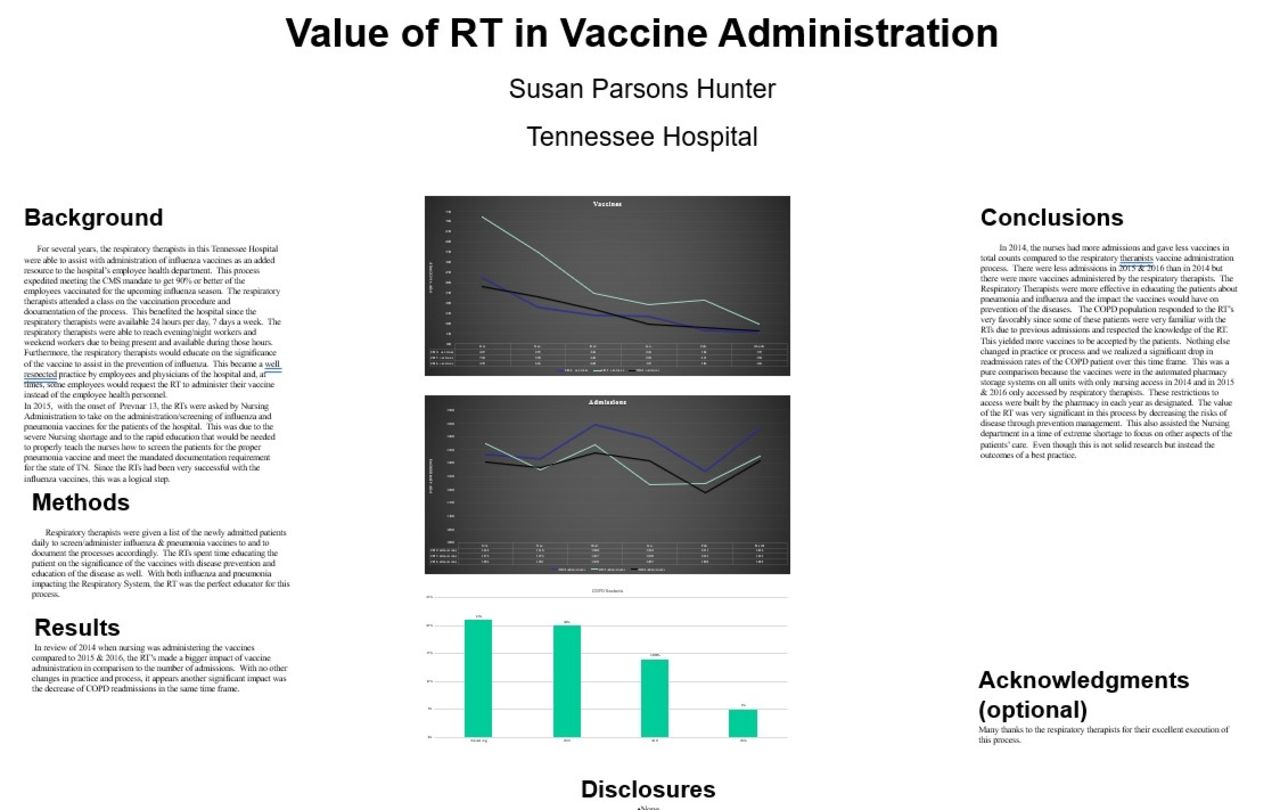
In 2015–2016, RTs made a bigger impact of vaccine administration in comparison to the number of admissions than the nurses in 2014. With no other changes in practice and process, decrease of COPD readmissions were also found.
Conclusions:
In 2014, the nurses had more admissions and fewer vaccines in total counts. There were less admissions in 2015–2016 than in 2014 but there were more vaccines administered by the RTs. The RTs were effective educators. The COPD population responded to the RTs favorably since some patients were very familiar with the RTs due to previous admissions and respected the knowledge of the RT. This yielded more vaccines to be accepted. Nothing else changed in practice or process and we had a drop in COPD readmission rates over this time frame. This was a pure comparison because the vaccines were in the automated pharmacy storage systems on all units with only nursing access in 2014, and in 2015–2016 only RT access. The value of the RT was significant in this process. Even though this is not research, it is outcomes of best practice.
Get full access to this article
View all access options for this article.