
Abstract
Background:
High frequency percussive ventilation (HFPV) is a time cycled, set flow, entrainment ventilator that delivers sub physiologic tidal volumes at percussive rates at or exceeding 500 bpm. HFPV is biphasic, separating it from other high frequency therapies. Gas is driven through a phasitron, described as a unique venturi that acts as a clutch mechanism. Until recently, all HFPV was facilitated with a proximal phasitron that attached directly to the patient’s airway. Proximal phasitron entrained heated and humidified gas through entrainment ports but lacked capability to fully compensate for dry driving gas. Introduction of the distal phasitron allows for HFPV gases to become heated and humidified to physiological standards. We hypothesized that, due to the distal position of the phasitron and attenuation through heated wire circuits, the distal phasitron is inferior compared to the proximal phasitron position.
Methods:
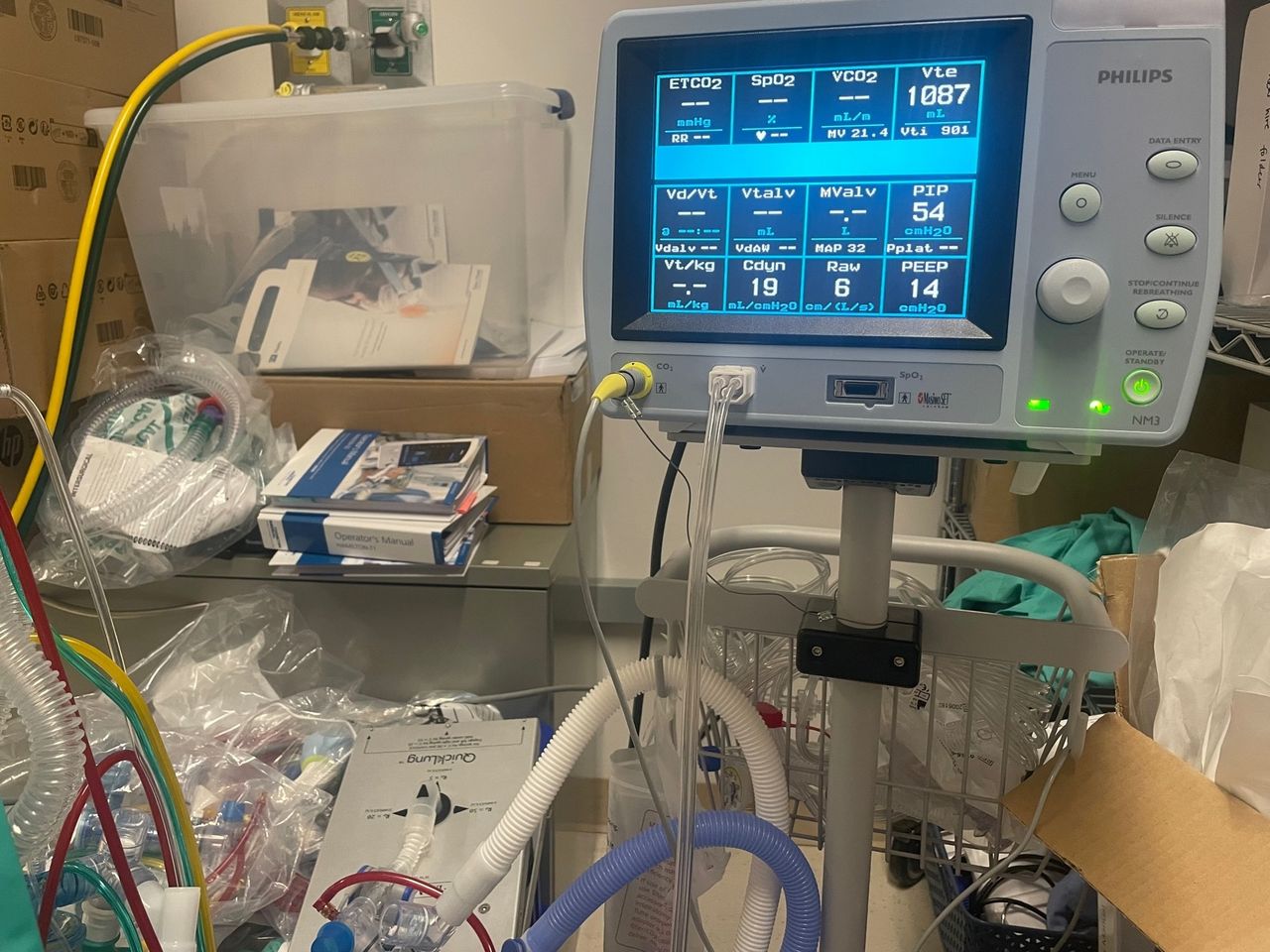
We compared phasitron function utilizing the Respironics NM3 respiratory monitor. Monitoring cuvette was placed in-between an Ingmar QuickLung and study circuits. The test lung was set for two different compliance (C = mL/cm H2O) and resistance settings (Rp = cm H2O/L/s), with replicate ventilator flow settings to target PIP and replicate PEEP flow knob dial positions. We utilized four specific models. Model 1 utilized C = 20, Rp = 5, and target PIP 50. Model 2 utilized C = 20, Rp = 5, and target PIP 60. Model 3 utilized C = 10, Rp = 20, and target PIP 50. Model 4 utilized C = 10, Rp = 20, and target PIP 70. Data was recorded and analyzed comparing differences in mean.
Results:
When comparing proximal and distal placement of the phasitron we found insignificant differences in measured values PIP, Raw, and VTe. Mean difference in PEEP found proximal placement increase by 12.5% compared to distal placement. Model 2 distal placement demonstrated a 6 cm H2O increase in PEEP over proximal placement and Model 4 distal placement showed a decrease in delivered PEEP by 14 cm H2O.
Conclusions:
Small sample size limited our ability to demonstrate statistical significance. PEEP variation in Model 2 and Model 4 were clinically significant. Under conditions of high Raw and poor compliance, the distal phasitron lacked the ability to maintain PEEP as compared to proximal position. On the contrary, with normal Raw and moderate compliance the distal phasitron increased PEEP as compared to the proximal positioning. More research is warranted to discover the mechanisms responsible for the variations.
VDR controls and distal phasitron QuickLung, Respironics NM3, and proximal phasitron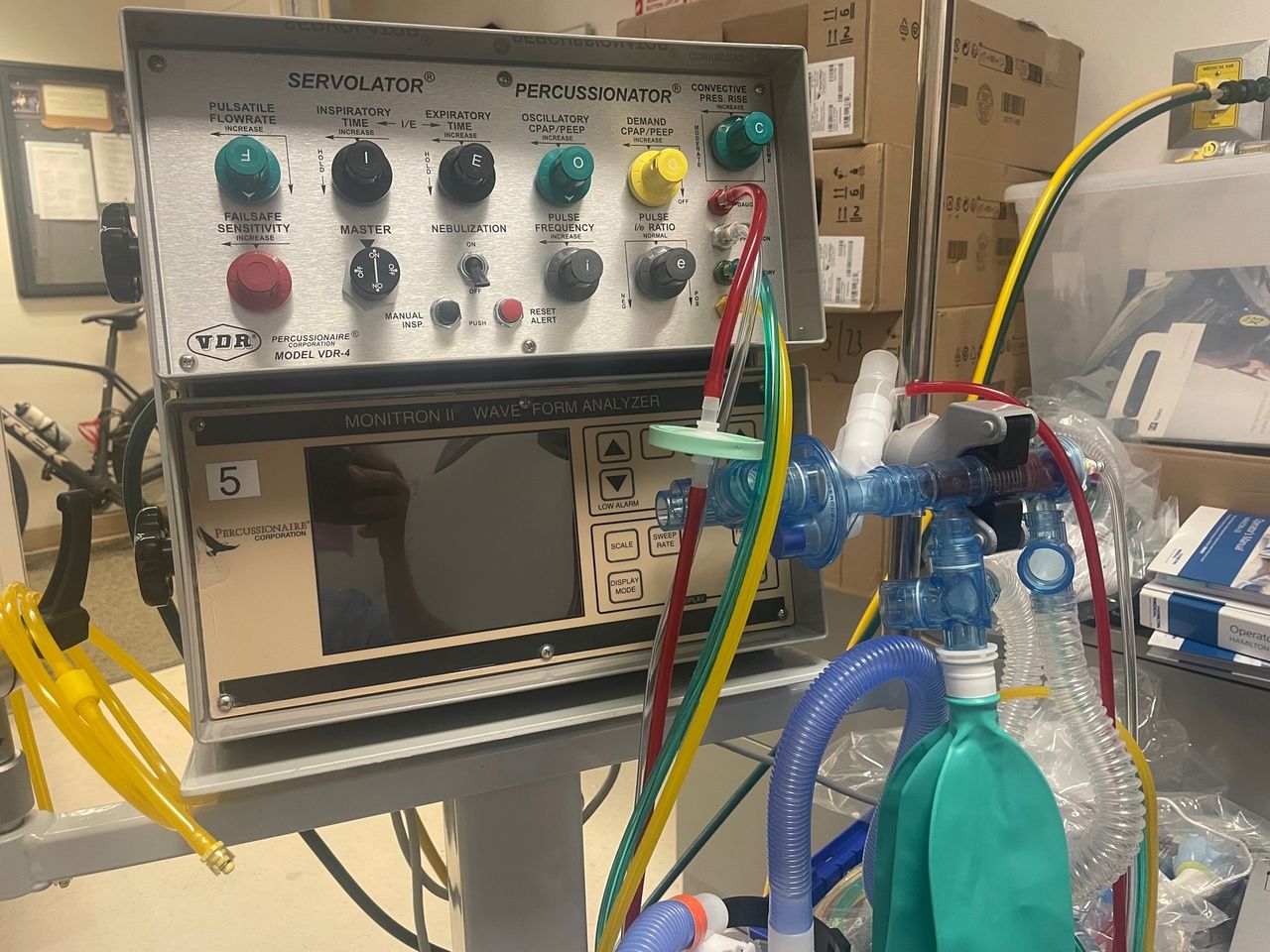
Get full access to this article
View all access options for this article.