
Abstract
Background:
Inspiratory synchronized vibrating mesh nebulizer (iVMN) has been reported to improve aerosol delivery during mechanical ventilation in adult models. A prototype VMN generating smaller aerosol particles than conventional VMN was developed. We aimed to compare the delivery efficiency of small and standard aerosol particles with an iVMN prototype and conventional controller during neonatal and pediatric mechanical ventilation.
Methods:
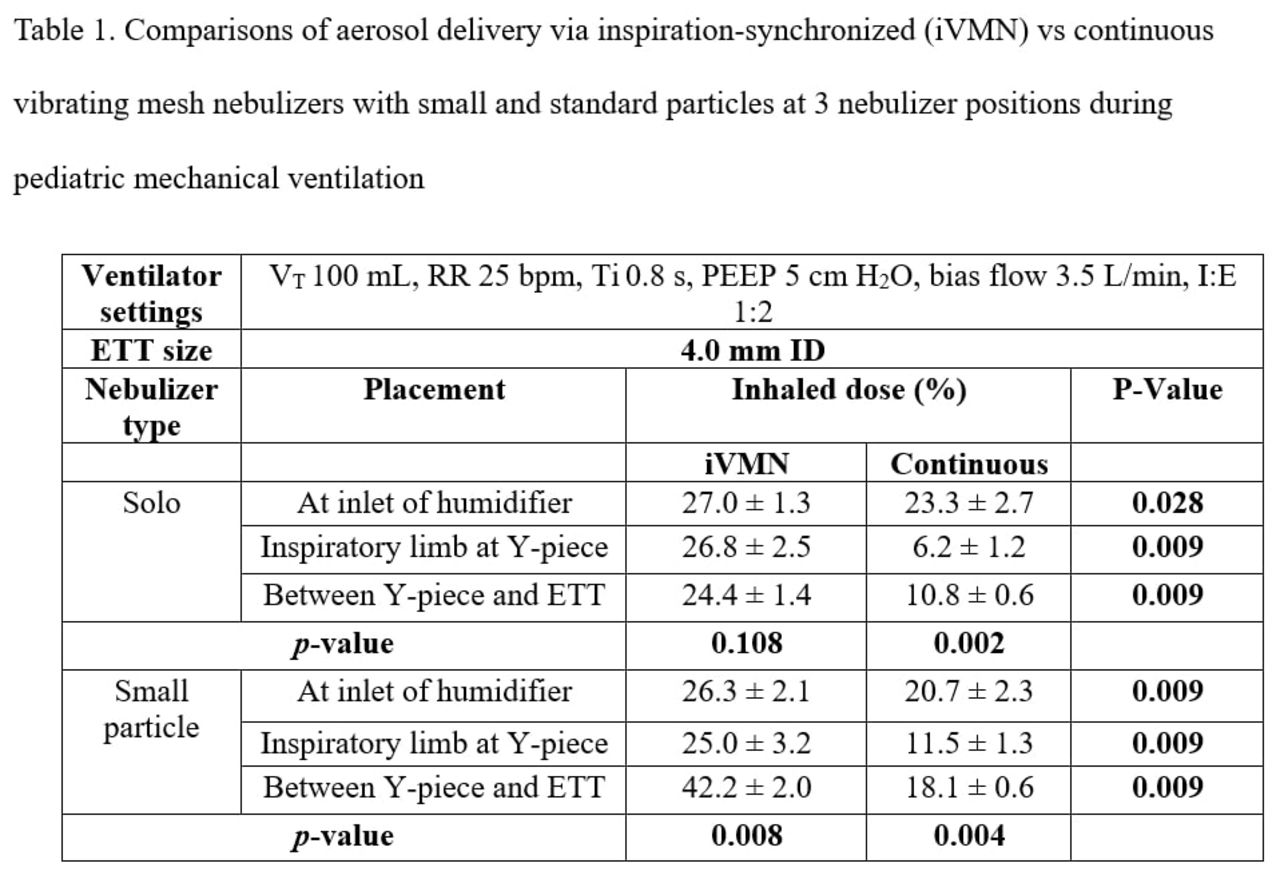
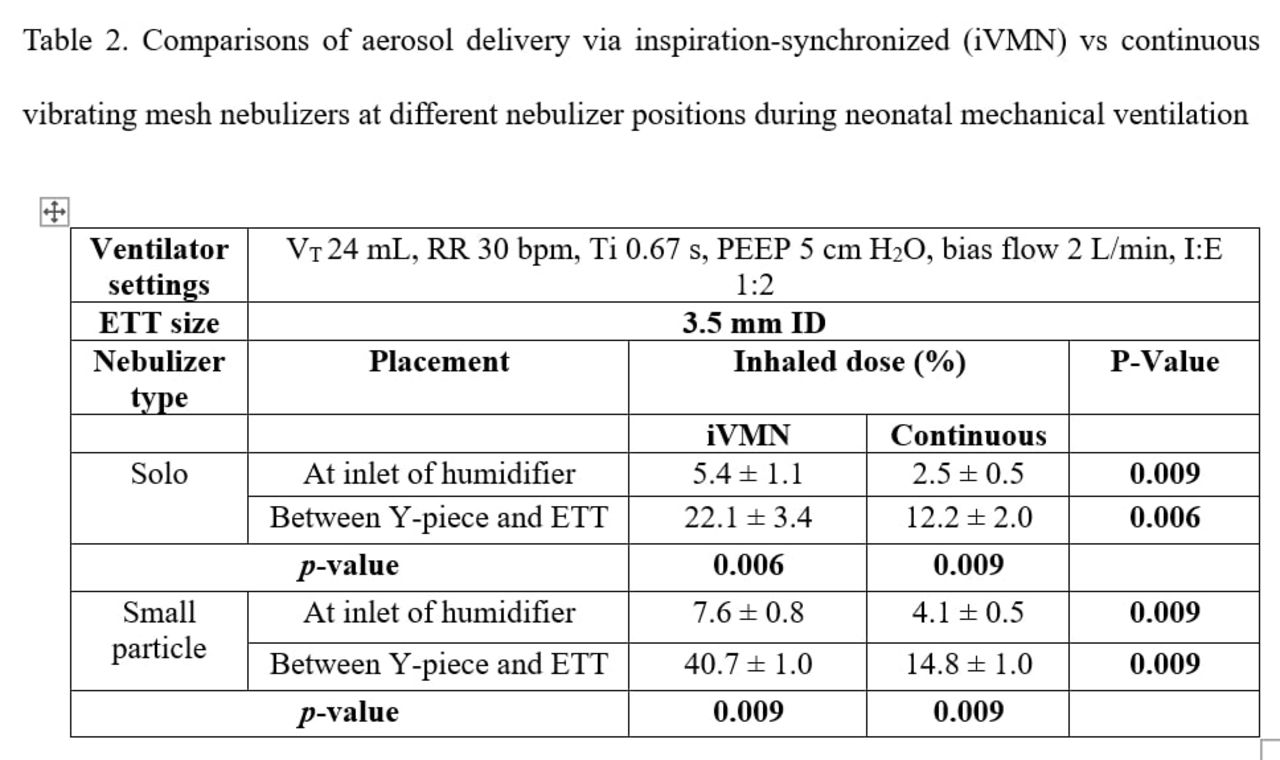
A critical care ventilator with heated ventilator circuit (pediatric and neonatal) was connected to an endotracheal tube (ETT) attached to a collecting filter and passive test lung. Set parameters for pediatric was volume control (VC) , VT 100 mL, frequency 25 breaths/min, Ti 0.8 s, PEEP 5 cm H2O, bias flow 3.5 L/min, I:E 1:2 and ETT 4.0 mm ID. Set parameters for neonate was VC, VT 24 mL, frequency 30 breaths/min, Ti 0.67 s, PEEP 5 cm H2O, bias flow 2 L/min, I:E 1:2 and ETT 3.5 mm ID. 1mL of albuterol (2.5 mg/mL) was administered with prototype small particle and conventional VMN, in iVMN and continuous mode, placed at inlet of humidifier, inspiratory limb at Y-piece, and between the Y-piece and ETT (n = 5). Albuterol was eluted from the collection filter and assayed with UV spectrophotometry (276 nm).
Results:
Percent of albuterol dose inhaled (mean ± standard deviation) are shown in Table 1, 2. Compared to continuous VMN, iVMN generated higher inhaled dose in both neonatal and pediatric mechanical ventilation, regardless of nebulizer placement and particle sizes (all P <.05). During neonatal mechanical ventilation, inhaled dose was higher with VMN placed between ETT and Y-piece than at the inlet of humidifier, regardless of aerosol generating modes and particle sizes (all P <.05). During pediatric mechanical ventilation, the inhaled dose was highest with continuous VMN placed at the inlet of humidifier. When iVMN was used, the inhaled dose was highest with small-particle VMN placed between ETT and Y-piece and no significant differences in conventional VMN placements. Small-particle VMN outperformed conventional VMN only when nebulizer was placed between ETT and Y-piece.
Conclusions:
During neonatal mechanical ventilation, aerosol delivery was higher with nebulizer placed between ETT and Y-piece than inlet of humidifier, regardless of the aerosol generating modes and particle sizes. During pediatric ventilation, highest aerosol delivery was achieved with continuous VMN placed at the inlet of humidifier and small particle iVMN placed between ETT and Y-piece.
Get full access to this article
View all access options for this article.