
Abstract
Background:
The COVID-19 pandemic caused a multitude of supply chain shortages. In our institution, this manifested as an inability to procure pediatric tracheostomy tubes (TT) made from medical grade silicone. A multidisciplinary team evaluated supply inventory and availability in our hospital (244 bed pediatric hospital, Level 1 Trauma Center, Level IV NICU) and multiple countermeasures were put in place to optimize inventory management while protecting patient safety. We aim to evaluate the cost implications and patient impact driven by the TT supply chain challenges.
Methods:
Absent of supply chain challenges the standard process in our institution included placement of a bundle of 4 TT (3 same size, 1 half size smaller). We reduced this bundle to 3 TT (2 same size, 1 half size smaller) to help conserve supply and limit costs. An SBAR notifier (Figure 1) was sent out to all patient care areas to inform providers of the change. Planned TT changes were prioritized M-F 6am-1pm to facilitate timely turnaround. TT change frequency remained at the institutional standard (q1week); however, TT re-processing was changed to increase from 5 to unlimited occurrences with a passed pre-bedside functional test. In an IRB approved retrospective analysis of all admitted trach patients from December 2021-April 2023, we analyzed 1008 trach patient encounters for safety events and average cost before and after our policy change of decreasing trach tubes in February 2022.
Results:
There was not a statistically significant (P < 0.05) increase in code blue, rapid response, emergent trach changes, or delays in care/incident reports pre (521 patients) and post (487 patients) TT stocking process change. On average, the cost before decreasing TT at bedside was $481,467.68 compared to $386,311 post bedside inventory reduction, a 19.7% decrease. A 337% increase in custom TT during the post period limited further potential cost reductions.
Conclusions:
A decrease in the number of bedside TT from four to three did not increase adverse events for pediatric hospitalized pediatric patients with tracheostomy tubes. The decrease in quantity stocked for emergent use at the bedside also decreased costs and can be considered safe with proper planning. Further research must be done related to supply chain inventory management and bedside emergency stock utilization.
Figure 1 displays the SBAR messaging that was sent to all inter-disciplinary staff that assume care of tracheostomy tube patients when the bedside inventory was reduced.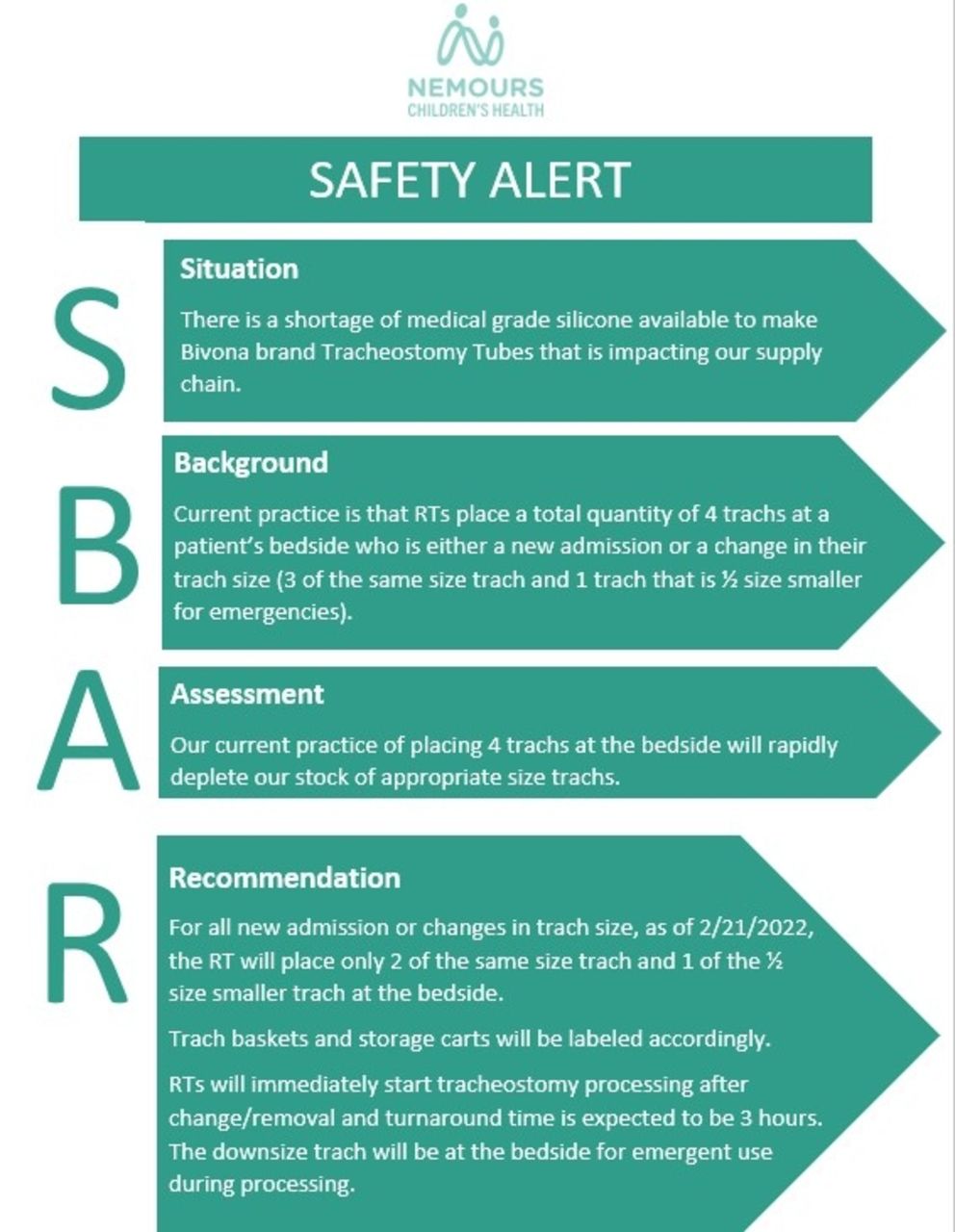
Get full access to this article
View all access options for this article.