
Abstract
Background:
During the COVID-19 pandemic, we have implemented automated oxygen titration (AOT) to optimize oxygen management and reduce the interventions from healthcare workers. We report here our experience at the emergency department (ED) in patients with suspected or confirmed COVID-19.
Methods:
We retrospectively collected data from the automated oxygen titration device (O2 flow, SpO2, SpO2 target, frequency, and heart rate) in patients managed with AOT at the ED between April 2021 and February 2022. We analyzed the oxygenation parameters (time within the SpO2 target, with hypoxemia and with hyperoxemia), the rate of partial or complete weaning. We evaluated the impact of the SpO2 target on oxygen flow when the target was modified by the clinicians by 2% or more.
Results:
We included 81 patients (mean age 72 ± 16 years, 57% were men) with suspected (n = 66) or confirmed (n = 15) COVID-19 requiring oxygen therapy. The mean duration of utilization of automated oxygen titration device was 14.3 ± 4.7 hours. A SpO2 signal was present 91.9% of the time. Main SpO2 targets set by the clinicians was 90%. Oxygen weaning was possible in 35/81 patients (36%). For the whole population/COVID-19 patients, the time in the SpO2 target was 78/81%, time with hypoxemia was 3/3%, time with hyperoxemia was 2/0.6%. In a subgroup of 11 patients with two different SpO2 targets (mean of 91.9 vs. 89.5%), the mean initial and final oxygen flow were 3.3 ± 0.6 and 1.9 ± 0.6 L/min respectively, P = 0.0076.
Conclusions:
In patients with acute respiratory failure, the utilization of automated oxygen therapy was feasible to manage patients with suspected or confirmed COVID-19. Similar to other studies with automated oxygen therapy, the time in the oxygenation target was high, and oxygen weaning was possible in 1/3 of the patients. The choice of the SpO2 target has a significant impact on oxygen flows.
Impact of the SpO2 target on oxygen flow in a subgroup of 11 patients with modified target. With high SpO2 target (mean 91.9%) reduced to low SpO2 target (mean 89.5%), oxygen flow was significantly reduced from 3.3 to 1.9 L/min.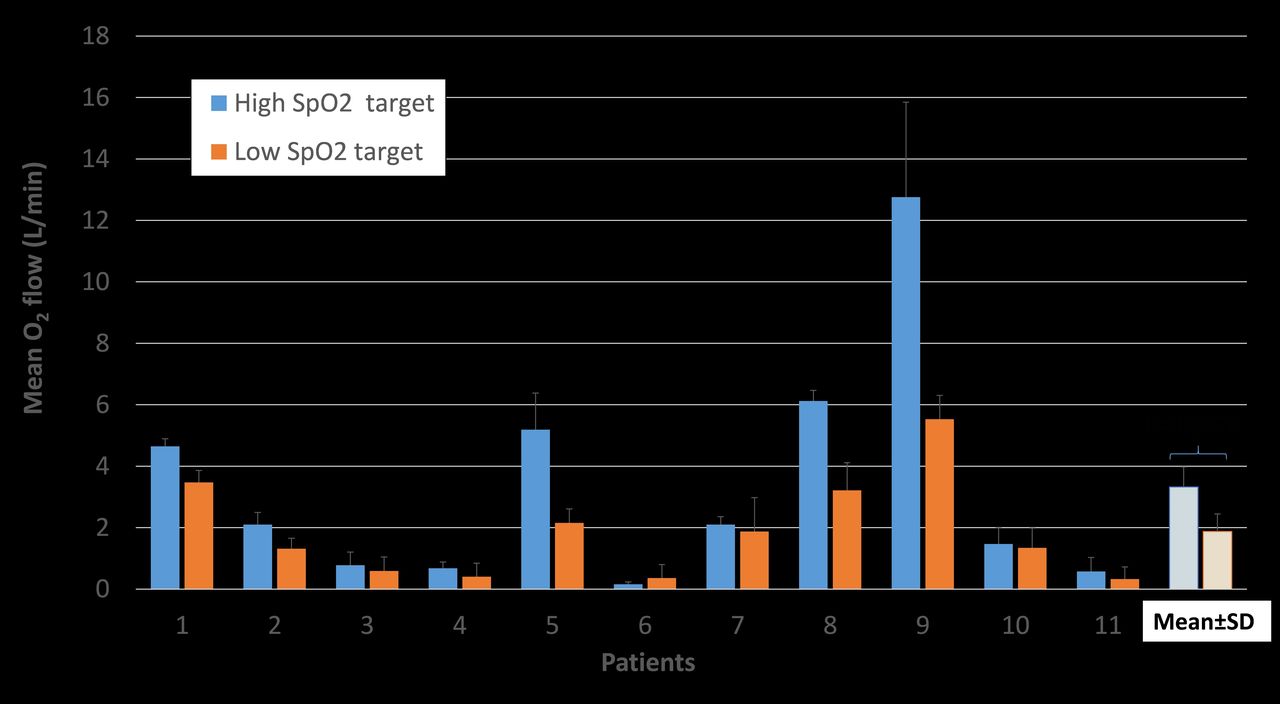
Get full access to this article
View all access options for this article.