
Abstract
Background:
Children with neurologic impairment (NI) hospitalized for pneumonia. Neurologic dysfunction and frequent comorbidities (ie, impaired cough, trach) in peds with NI contribute to increased risk of infection, altered epidemiology, and different treatment needs than peds without NI. Variation in pneumonia management and outcomes across pediatric hospitals for peds with NI led to development of inpatient pneumonia care recommendations. The objective is to increase the % of peds with NI hospitalized with pneumonia who received antibiotics and airway clearance therapies concordant with care recommendations on admission from 40% to 90% over 1 year.
Methods:
Our multidisciplinary team of clinicians, respiratory therapists (RTs), a pharmacist, and a research coordinator employed QI methods to implement antibiotics and airway clearance care recommendations. A process map identified reasons for failures and informed key drivers: knowledge of care recommendations, process standardization, effective communication, identification and mitigation of failures, and stakeholder buy-in. Our primary measure was concordance with antibiotics and airway clearance recommendations in the first 24 hrs of hospitalization and was determined by patient medical history (ie, pneumonia, prior cultures, home airway clearance) and review of therapies provided. Multiple plan-do-study-act cycles were completed for interventions: education, airway clearance reference table, standardized RT evaluation, EHR order sets, and provider feedback. We tracked the impact of interventions over time using a run chart with established rules for special cause. Given relative infrequency of hospitalizations, we examined data in groups of 5 patients.
Results:
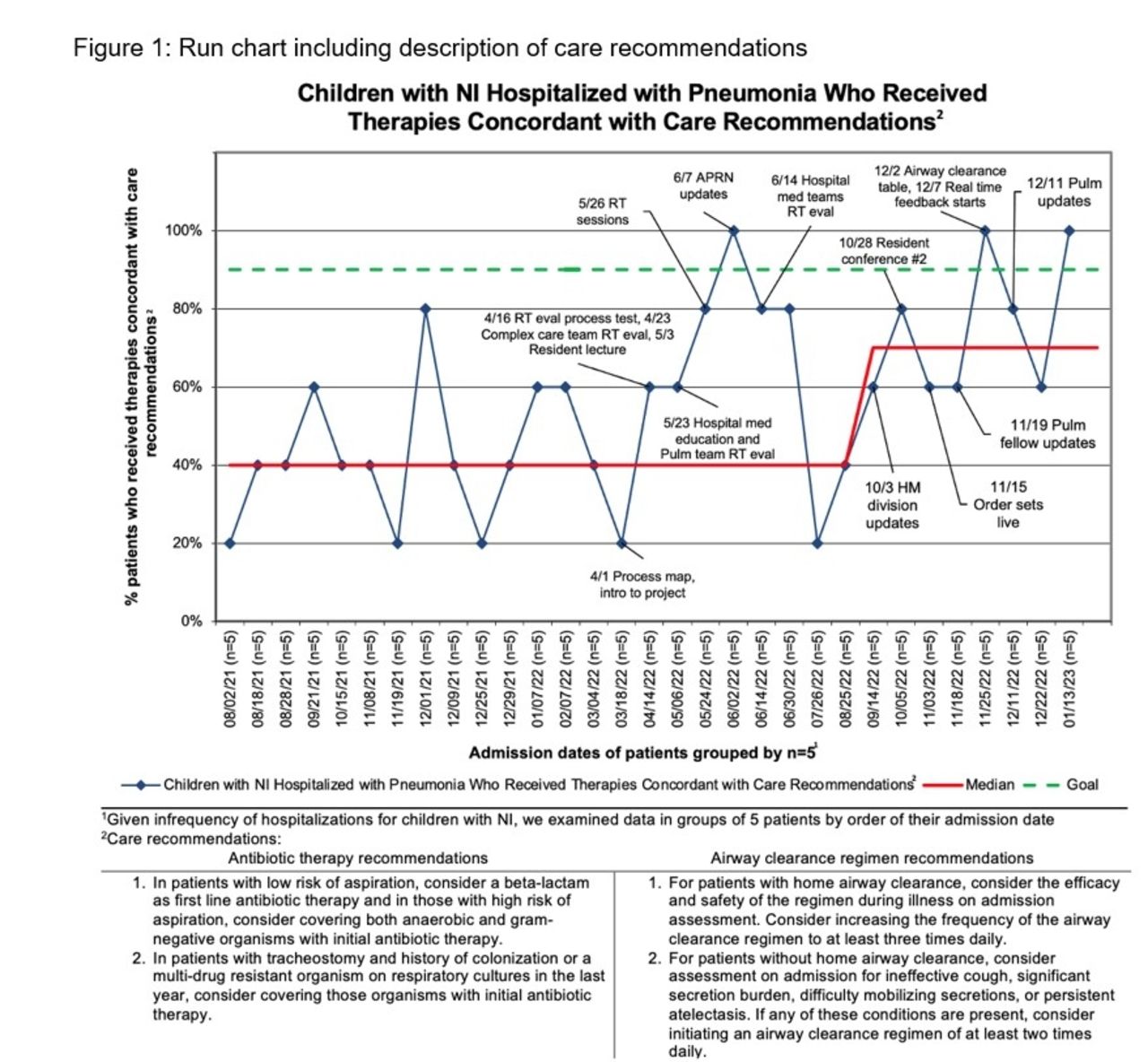
The median percentage of children with NI hospitalized for pneumonia receiving therapies concordant with care recommendations on admission increased from 40% to 70% over the first 6 months with sustained change over 4 additional months (Figure 1).
Conclusions:
QI methodology with a focus on multidisciplinary collaboration led to improved adherence to care recommendations for pneumonia in hospitalized children with NI. Education, changes to facilitate consistent RT workflow, and optimized communication influenced adherence, while order sets allowed for sustained change in our system. Next steps include study of patient outcomes associated with care recommendation adoption.
Get full access to this article
View all access options for this article.