
Abstract
Background:
The need for an RT (respiratory therapist) trach/vent navigator position at Levine Children’s Hospital (LCH) was evaluated and determined necessary as readmissions for trach/vent dependent children were 10% higher than the national average. LCH had a readmission rate of 25-33% vs. 17-22% nationally (Yu et al, 2017). Upon evaluation, it was found that the standardization of teaching and preparing families for home with this patient population was lacking. The intent was to decrease readmissions, decrease length of stay, and improve patient outcomes. IRB approval was received as a quality improvement exemption.
Methods:
The pediatric pulmonary team and the RT department created a position for a dedicated pediatric RT to standardize teaching, aid in clinical decisions, and prepare families for home. The RT navigator role was created to improve care coordination for the trach/vent patient; acting as a go-between for the patient and the healthcare multidisciplinary teams. The navigator provides thorough education and a discharge plan that addresses the patient's individual respiratory care needs.
Results:
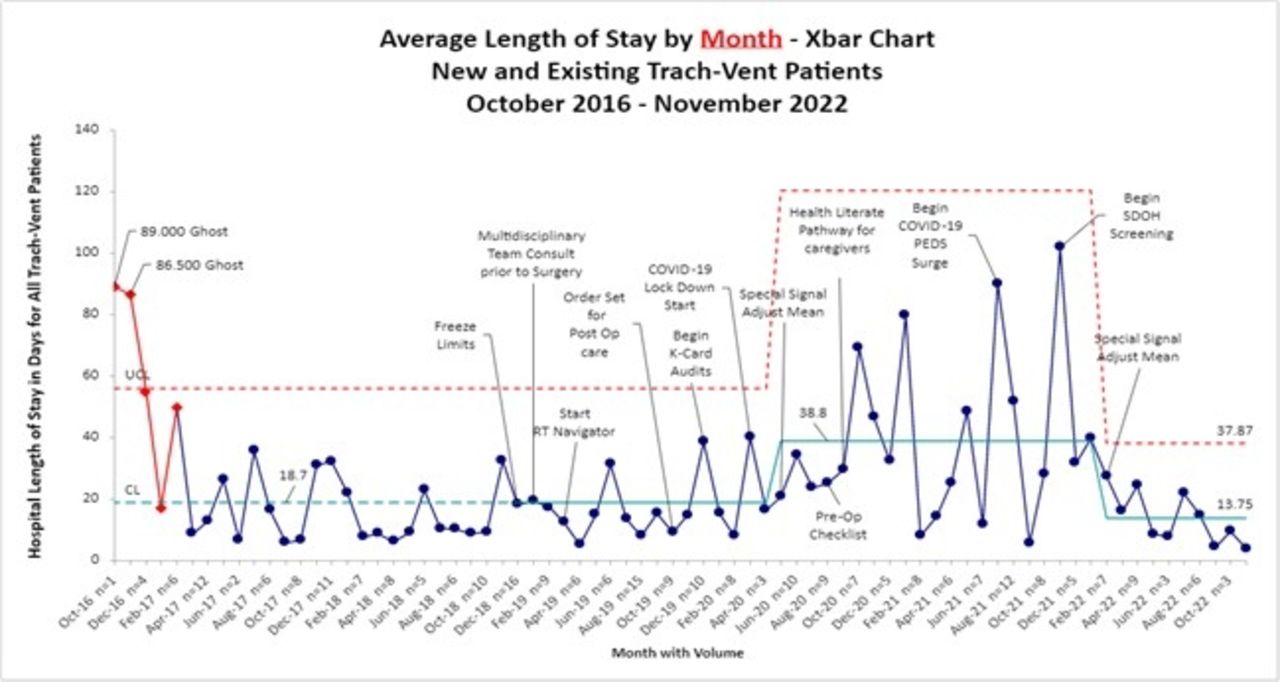
The RT navigator is like the role of the RT Discharge Coordinator described by Tearl et al, 2006 in that LOS was decreased from 82 + 45 and after implementation to 48 + 44 days. The length of stay chart shows the decrease after LCH implemented the role. In addition, readmissions decreased from 29.6% to 15%.This position has evolved into other supportive roles for both the pulmonary and respiratory teams. We conducted a staff survey regarding the RT navigator role and of 26 participants, 65% said they assisted with patient care and 88% agreed they are supportive with questions, pulmonary plan of care, and discharge goals. LCH conducted a survey for families based on their experience with the RT navigators in transitioning from hospital to home. The participants rated their confidence with trach changes and emergency scenarios on a scale of 1-10, with a reported average of 9.2. Of the information provided, 15 of 15 participants said yes to understanding the education provided by the RT navigators. The overall comments were positive, and families felt confident leaving the hospital to go home.
Conclusions:
As tracheostomy placement for pediatric patients becomes more common, the need for a dedicated RT navigator for families to discharge home has proven valuable. At our institution, we demonstrated a reduction in both LOS as well as readmissions. This was coupled with improved provider and family satisfaction.
Get full access to this article
View all access options for this article.