
Abstract
Background:
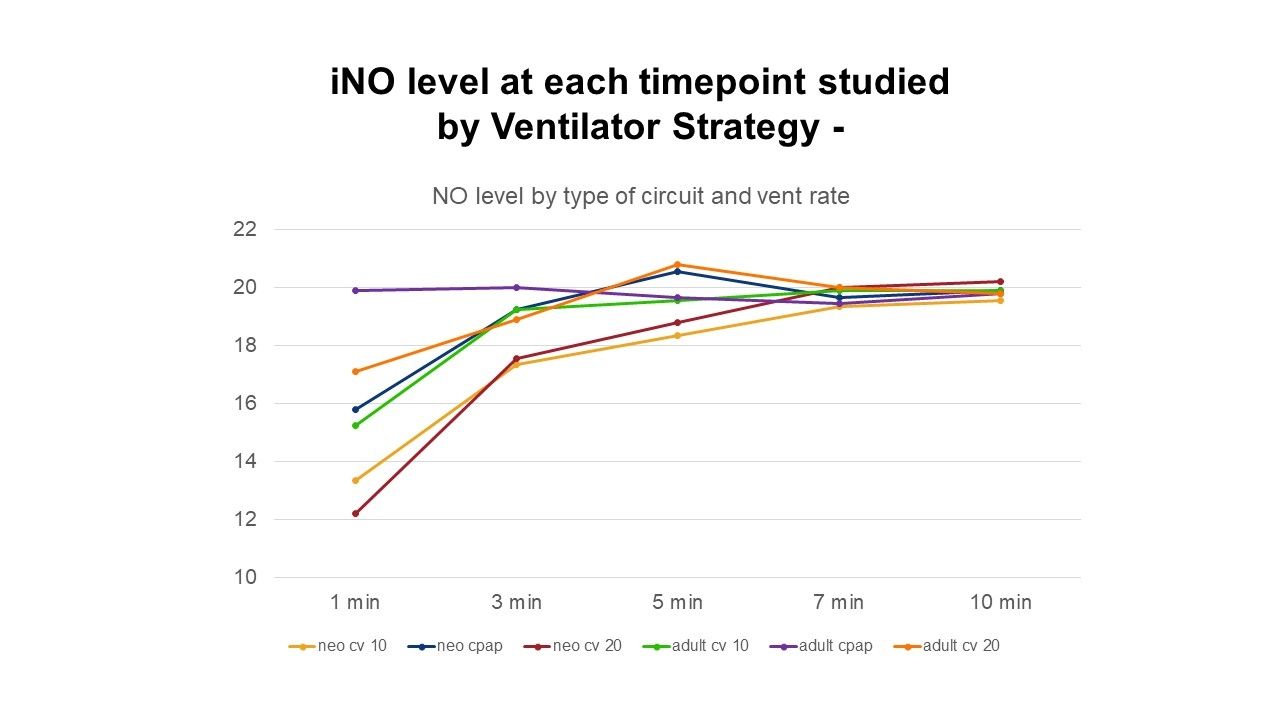
Inhaled Nitric Oxide (iNO) and Intrapulmonary Percussive Ventilation (IPV) are indicated in selected intubated patients with hypoxic respiratory failure and airway clearance therapy needs. Providing consistent iNO during IPV has been challenging. The purpose of this study is to determine the time to reach iNO concentration using the Genosyl Delivery System (Vero Biotech, Atlanta, GA) comparing adult and neonatal ventilator circuits, one IPV and three ventilator strategies.
Methods:
A Drager V500 ventilator (Drager, Telford, PA) was attached to RT380 (adult) and RT265 (neonatal) ventilator circuits (Fisher & Paykel, Irvine, CA). On the inlet side of a MR290 canister, a Genosyl adaptive flow sensor was attached to an injector adapter with disc filter and True IPV T with phasitron and the circuit. The vent circuit y-piece was connected to a BC Biomedical test lung (adult) and Infant Ingmar Neo Lung (Ingmar, Pittsburgh, PA) for the individual circuit tests. An IPV 1C (Percussionaire, Sandpoint, ID) was used for the IPV. The Genosyl DS was used to deliver and monitor measured iNO and NO2 parameters. The level of iNO in ppm was measured at 1, 3, 5, 7, 10 min using 54 trials: 27 neonatal and 27 adult circuit tests, using vent strategies of CPAP +5, PC f 10 20/5 and PC f 20 30/5, analyzed independently using IPV strategy f 100, PIP 25 and iNO set at 20 ppm. We compared the time to reach 20 ppm iNO using univariate (Wilcoxon rank sum test or one-way ANOVA for three groups comparisons for type of circuit (adult vs. neonatal) or vent rate (CPAP vs. rate 10 vs. rate of 20) or vent peak inspiratory pressure (10 vs. 20 vs. 30) respectively, and multifactorial ANOVA to examine all three variables independent association with time to reach 20 ppm comparing; significance set at P < .05.
Results:
The adult circuit reached 20 ppm iNO sooner than the neonatal circuit (median (IQR) 3 (3, 5) vs. 5 (3, 7), P = .02, by rank sum test. There was a statistically significant difference in time to reach 20 ppm iNO between a vent rate of 10 and CPAP P = .02; iNO reached 20ppm faster with CPAP. The level of PIP was not associated with any difference in time to reach iNO 20 ppm.
Conclusions:
Nitric oxide can safely be used clinically with in-line IPV therapy and safely reach and maintain a stable iNO dose during IPV treatment. Peak iNO concentration of 20 ppm was achieved earlier using an adult circuit in the CPAP mode during IPV therapy.
iNO, inhaled nitric oxide, IQR, interquartile range, CPAP, continuous positive airway pressure *P+0.02, by Wilcoxon rank sum test, **P=0.02, by one-way ANOVA, significance between CPAP and rate 10 by Bonferroni post-hoc test, P=0.018
View all access options for this article.
Table 1. Variables Studied
Time to reach 20ppm iNO in minutes (Median, IQR)
Circuit*Neonatal (n=27)Adult (n=27)
5 (3,7)3 (3,5)
Ventilator rate**Rate 0, CPAP (n=18)Rate10 (n=18)Rate 20 (n=18)
3 (1,5)5 (3,7)5(3,5)
Peak inspiratory pressure10 (n=18)20 (n=18)30 (n=18)
3 (3,5)5 (3,7)3 (3,5)
Get full access to this article