
Abstract
Background:
Homecare ventilators are used across an array of patients and diseases. Patient characteristics often determine best circuit configuration. We aimed to evaluate FIO2 delivery of two commonly used circuits with a low flow O2 source.
Methods:
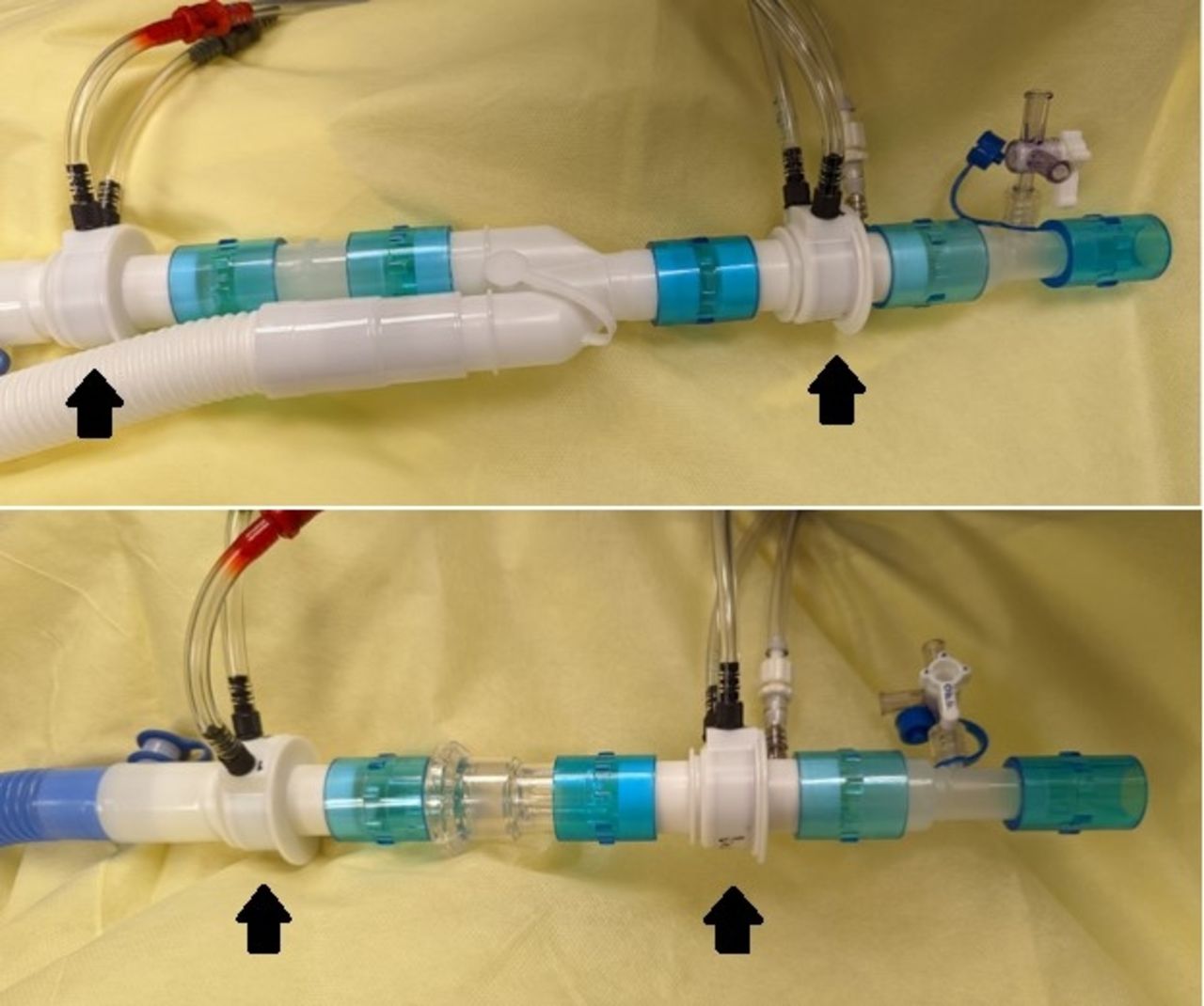
An Astral 150 ventilator in PS mode with two 22mm circuits was tested: dual limb active flow circuit (AFC) vs. single limb passive leak circuit (PLC) (Figure 1). Flow was measured using PowerLab with pneumotachometers placed at the inspiratory limb and y-piece (AFC) and proximal to leak port and at the y-piece (PLC). An ASL 5000 simulated an actively breathing 5 kg infant with BPD: C = 2 mL/cm H2O, Rin = 70 < Rout = 90 cm H2O/L/s, URC = 0.2 L, frequency = 40 breaths/min, sinusoidal pattern. O2 was bled in at 1 L/min increments from 1-6 L/min and FiO2 measured at the y-piece. Ten consecutive breaths for each run were analyzed. A two-way ANOVA evaluated the interaction of circuit type and O2 flow on FIO2 and two-sample t-tests compared FIO2 and flow between circuits.
Results:
A difference in FiO2 as a function of O2 flow and circuit type was observed, with significant interaction between the two (P < .001). Mean FIO2 was lower at each O2 flow using the PLC compared to the AFC (Table 1). When comparing O2 delivery for both circuits with similar FIO2 (1 L/min = 0.32, AFC and 4 L/min = 0.33, PLC) the L/min O2/peak inspiratory flow (PIF) ratio from the inspiratory limb (AFC) or proximal to the leak port (PLC) was of similar magnitude (0.073 vs 0.083, respectively). This was the result of higher PIF proximal to the leak port (48.1 ± 0.1 L/min) vs. the inspiratory limb of the AFC (13.6 ± 0.1 L/min)(P < .001). The difference in PIF between the inspiratory limb and y-piece of the AFC was 0.62 ± 0.31 L/min vs. 37.5 ± 0.46 L/min (P < .001) between proximal to the leak port and the y-piece for the PLC.
Conclusions:
An active lung model highlights considerations that must be made when choosing the appropriate circuit for patients. Higher FIO2 can be achieved at lower O2 flow when using an AFC vs. PLC because of the high flow required through the proximal portion of the PLC to compensate for intentional leak. While there was a statistical difference between L/min O2/PIF in the inspiratory limb (AFC) and proximal to the leak port (PLC), the ratios were of similar magnitude. Higher flow to compensate leak allows for delivery of prescribed settings; however, ability to achieve target FIO2 may be compromised. Feasibility and sustainability of high O2 flow must be weighed to optimize support, comfort, and safety.
Average FiO2 at each oxygen flow level for each given circuit configuration.
OXYGEN FLOW INPUT (L/MIN)
MEAN FIO2 ACTIVE FLOW CIRCUIT
MEAN FIO2 PASSIVE LEAK CIRCUIT
1
0.32
0.26
2
0.42
0.27
3
0.51
0.30
4
0.61
0.33
5
0.75
0.38
6
0.91
0.43
Get full access to this article
View all access options for this article.