
Abstract
Background:
More than 10% of full-term newborns require resuscitation after delivery due to delayed transition causing respiratory distress. Legacy Salmon Creek Medical Center handles approximately 300 deliveries per month. NICU admission is both expensive and requires separating infants from parents, causing distress and possible adverse effect on breastfeeding. Exploring whether a change to our delivery room respiratory management could decrease short-term stays by reducing initial admission rate. IPV therapy provides high frequency pulsatile flow to aid in secretion clearance and lung inflation. Our null hypothesis was that a 10-minute round of IPV would not impact short-term admission to the NICU.
Methods:
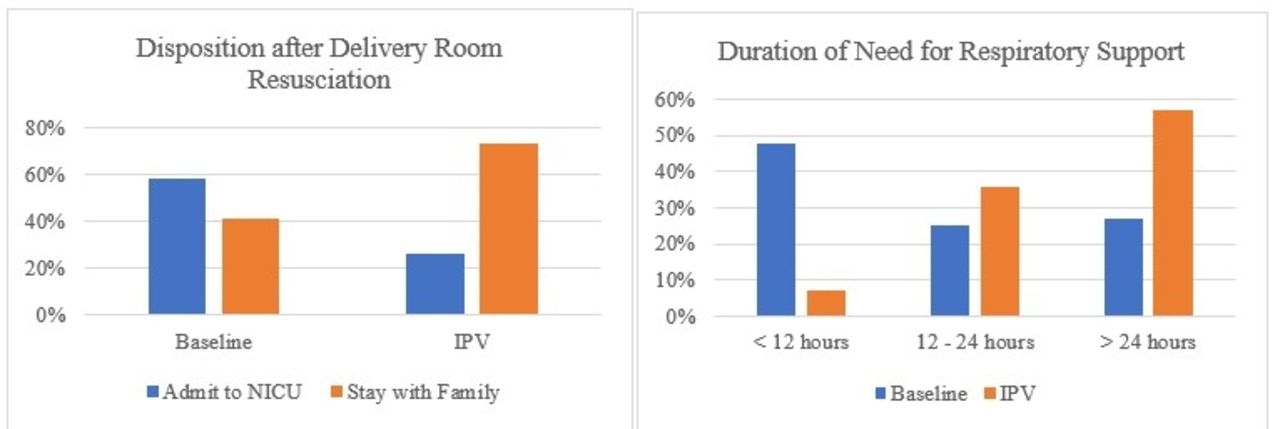
Baseline data was performed as follows: up to four 10-minute rounds of mask CPAP with assessment after each round of infant’s respiratory status on room air, work of breathing, and oxygen saturations. Post practice change, either the second (meconium aspiration) or third (all others) round of CPAP was replaced with 10 min of IPV therapy for babies ≥36 weeks gestational age. IPV therapy was recorded, and a retrospective analysis was done by the neonatologist. Baseline NICU admission rate reviewing the 121 infants that required >30 min of mask CPAP in the year leading up to the practice change. 59% of those patients were admitted to the NICU while 41% were effectively transitioned and remained with their mothers.
Results:
Analysis conducted after 6 months; 53 patients treated with IPV therapy 14 (26%) admitted to the NICU, a 55% decrease (P < .001) from the baseline rate of 59%. Infants who required admission after receiving IPV typically required >24 hours (often 3–4 days) of respiratory support indicating underlying pathophysiology that could not be relieved by delivery room intervention. A significant reduction in short term stays as only 7% of infants admitted after IPV required <12 hours of CPAP compared to 48% of the baseline group. Safety was demonstrated by no increase in pneumothorax rate in infants receiving IPV.
Conclusions:
IPV therapy in the delivery room performed with the IPV 2C was found to be safe and effective in aiding in transition to extrauterine life by alleviating transitional respiratory distress and reducing short-term NICU admissions. Reduction of these admissions and the potential need for transport to a medical center with a NICU benefits patients and families by keeping them together, in addition to reducing costs for facilities.
Get full access to this article
View all access options for this article.