
Abstract
Background:
The AirLife Open Mask made by Vyaire (Mettawa, Il) specifies that it delivers an FIO2 range of 0.24-0.9 between 1-15 L/min. This study aims to test if changes in patient inspiratory flow demand affect the FIO2 delivery of the mask. We hypothesize that there is no difference in the FIO2 delivery of the Vyaire AirLife Open Mask when compared to the manufacturers claimed FIO2 delivery.
Methods:
The AirLife Open Mask was attached to an intubation trainer mannequin (Laerdal Medical, New York) and ASL 5000 (Ingmar Medical, Pittsburgh, Pennsylvania) breathing simulator. The mannequin’s trachea was connected to the simulator using a T adapter, and an Ohio Medical Mini-Ox (Ohio Medical, Gurnee, Illinois) O2 analyzer was used to obtain an FIO2 reading in the trachea. The ASL simulator was set up at three different inspiratory flow demands, to include a normal breathing pattern with a VT of 500 mL, frequency 12 breaths/min, and TI of 1 s; second, was a hypoventilation pattern with a VT of 300 mL, frequency 8 breaths/min, and TI of 1.5 s; and third was a hyperventilation pattern with a VT of 700 mL, frequency 22 breaths/min, and TI 0.6 s. For each breathing pattern, the oxygen flow set to the mask was 1 L/min, 7 L/min, and 15 L/min respectively. The simulator was allowed to run until the VT was stable and the FIO2 for each scenario was recorded once the measurement reached equilibrium. Each breathing pattern and set flow combination was performed in triplicate. The O2 analyzer was calibrated between each run.
Results:
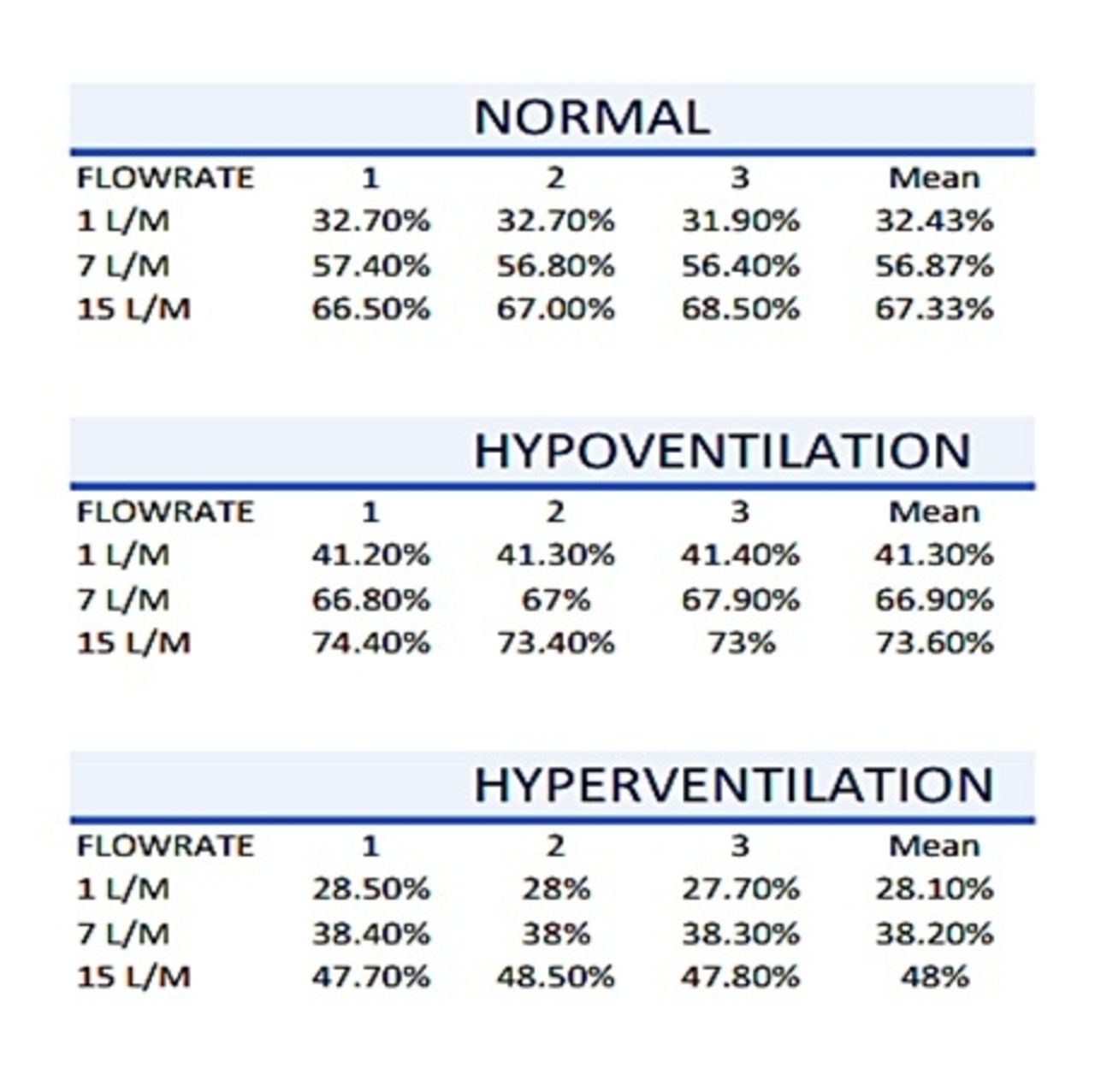
The normal breathing pattern resulted in a mean FIO2 of 32.43% at 1 L/min, 56.87% at 7 L/min, and 67.33% at 15 L/min. The hypoventilation pattern resulted in a mean FIO2 of 41.3% at 1 L/min, 66.9% at 7 L/min, and 73.6% at 15 L/min. The hyperventilation pattern resulted in a mean FIO2 of 28.1% at 1 L/min, 38.2% at 7 L/min, and 48% at 15 L/min.
Conclusions:
This study demonstrated that the mean FIO2 was highest with a reduced inspiratory flow demand across all set O2 flows. It was also found that mean FIO2 delivered to the trachea significantly decreased with increased inspiratory flow demand. Based on the above, our hypothesis is rejected. The FIO2 delivered to the trachea was decreased when compared to the manufacturers claims in the product insert and associated brochures at 15 L/min across all breathing patterns. It performed well at set flows of 1 L/min and 7 L/min during the normal and hypoventilation breathing patterns, however, it underperformed at all set flows during the hyperventilation breathing pattern.
Get full access to this article
View all access options for this article.