
Abstract
Background:
Awake prone positioning (APP) has been reported to improve oxygenation and reduce the need for intubation in patients with acute hypoxemic respiratory failure (AHRF). However, the impact of APP on ventilation distribution during various forms of respiratory support remains uncertain.
Methods:
Thirty-four patients were consented and included in this study after obtaining IRB approval (No. B2022-359R). The patients underwent 30-min phases of each respiratory support device in both supine position (SP) and APP in a random sequence. The respiratory support devices included high-flow oxygen mask (HFOM) at 60 L/min, high-flow nasal cannula (HFNC) at 60 L/min, and CPAP at 8 cm H2O. FIO2 was adjusted to maintain SpO2 at 90-95%. Ventilation parameters including global inhomogeneity (GI) index, center of ventilation (COV), ROI (region of interest), and dorsal fraction of ventilation were continuously assessed using electrical impedance tomography (EIT).
Results:
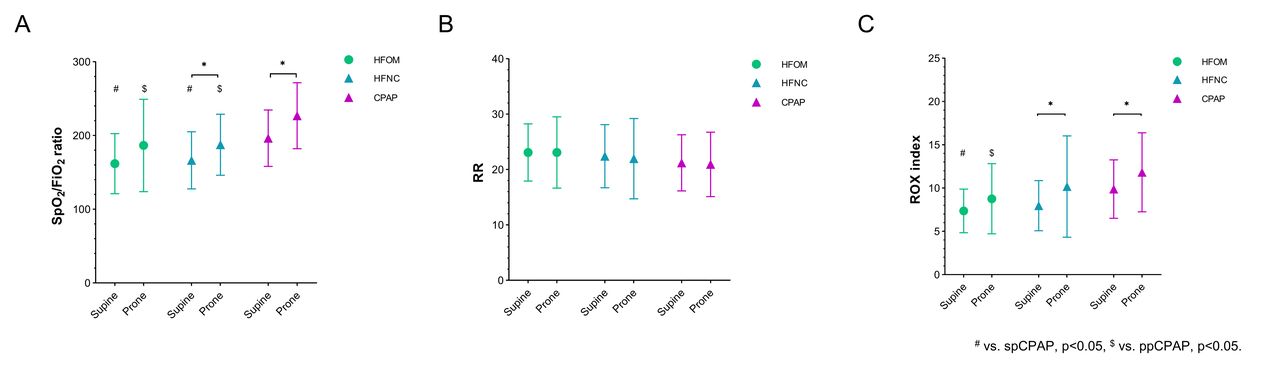
Among the 34 patients, 24 were male, age 73 ± 10 years, with an average body mass index (BMI) of 25 kg/m2. The average APACHE II score at enrollment was 13 ± 4. The SpO2/FIO2 ratio, ROX index (SpO2/FIO2 ratio/breathing frequency), and GI index were higher in APP compared to SP, regardless of respiratory support devices used (all P < .05). Similarly, these variables were higher with CPAP than HFOM and HFNC, regardless of patient positions (all P < .05). There was no significant interaction observed between body position and respiratory support. In the supine position, the COV with CPAP (53.4 ± 8.1%) was higher than that with HFOM (47.8 ± 6.0%, P = .015) and HFNC (48.1 ± 7.2%, P = .030). However, the COV with CPAP decreased to 46.7 ± 7.1% during PP (P = .001). With the use of CPAP, the ventral ventilation significantly increased during APP (44.9 ± 15.0 vs 55.0 ± 19.9%, P = .017), predominantly in layer ROI 1(6.9 ± 6.2 vs 11.5 ± 9.9%, P = .022), while a significant decrease was observed in layer ROI 3(48.0 ± 12.2 vs 39.6 ± 16.3%, P = .020). Additionally, significant discomfort was reported in both APP and with the use of CPAP.
Conclusions:
Compared to HFOM and HFNC, CPAP significantly improved oxygenation but may lead to overdistention, while the use of APP during CPAP facilitated homogeneous ventilation distribution and further improved oxygenation. However, patient tolerance may decrease when these interventions were employed.
Evolution of ventilation distribution(%) in the horizontal regions of interest (ROIs) during HFOM(A), HFNC (B), CPAP (C) and Global inhomogeneity index(D), Center of Ventilation(%) (E) was evaluated in both supine and prone position. * P<0.05, # vs. spCPAP, p<0.05, $ vs. ppCPAP, p<0.05. Comparisons of SpO2/FiO2, Respiratory rate(RR) and ROX index were assessed during HFOM, HFNC, CPAP in both supine and prone positions. * P<0.05, # vs. spCPAP, p<0.05, $ vs. ppCPAP, p<0.05.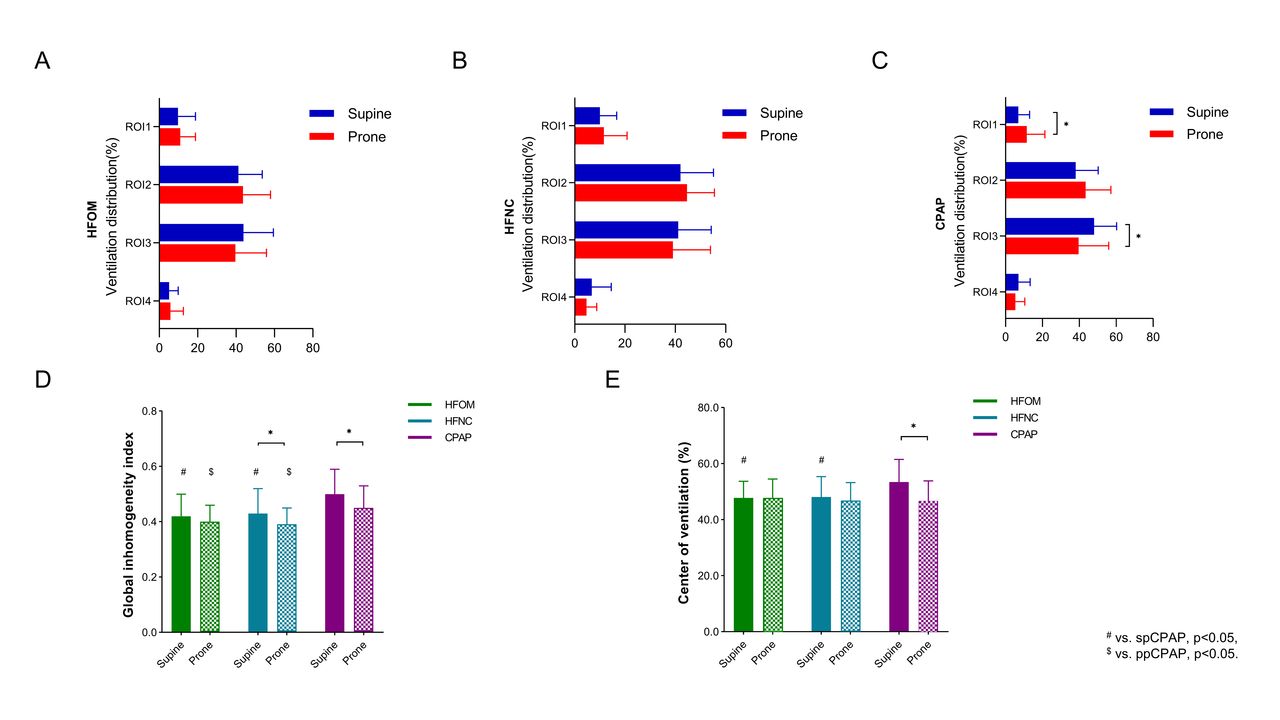
Get full access to this article
View all access options for this article.