
Abstract
Background:
Many spontaneous breathing tracheostomized children receive inhaled medications, but the optimal aerosol delivery methods for them remain unclear. We aimed to assess the impact of different humidification devices and flow settings on aerosol delivery for spontaneously breathing tracheostomized infants and toddlers.
Methods:
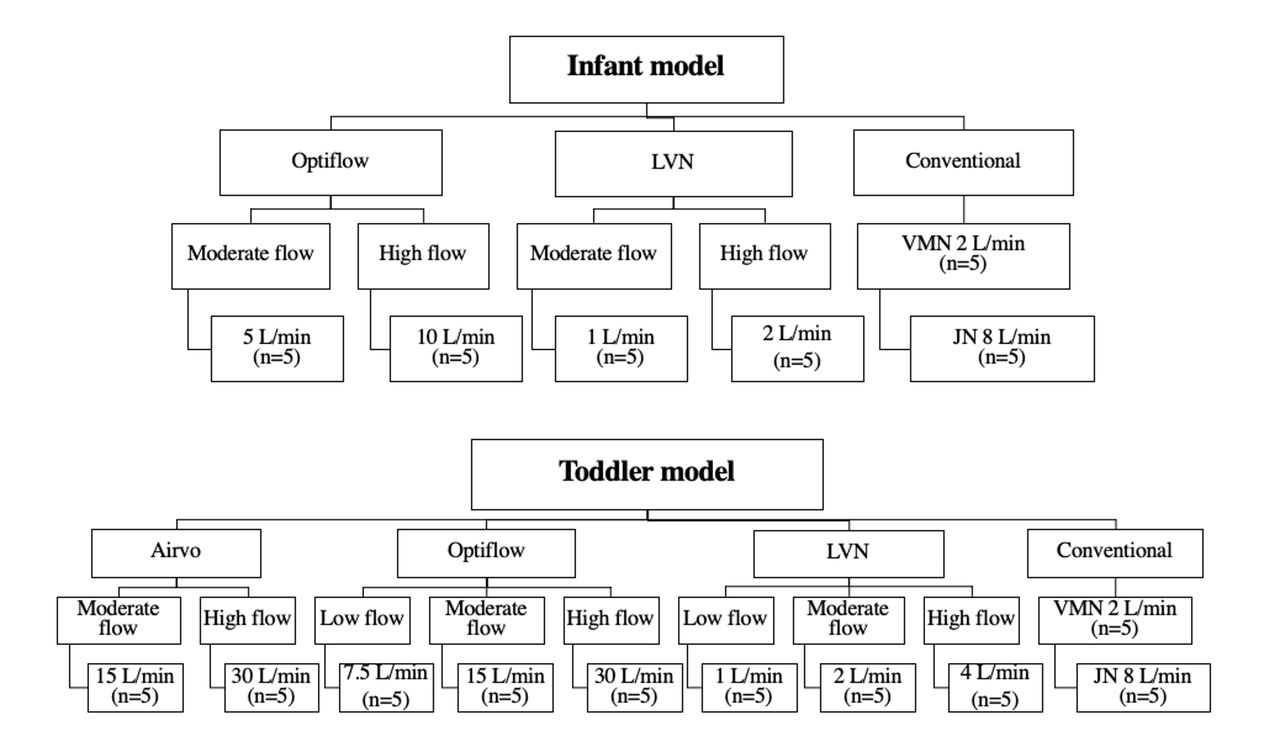
Spontaneous breathing models of trached infant (5 kg) (tidal volume [VT] 30 mL, breathing frequency 30 breaths/min, inspiratory:expiratory [I:E] 1:2.3, and trach size 4.5 mm) and toddler (15 kg) [VT 100 mL, frequency 20 breaths/min, I:E 1:2.3, and trach size 5.5 mm) with a collecting filter placed distal to the airway. Albuterol sulfate (2.5 mg/3 mL) was administered via a vibrating mesh nebulizer (VMN) in all conditions with heated and unheated humidification. VMN was placed near the humidification device and compared in different settings: 1) Optiflow set at 37°C and flows of 5 vs. 10 L/min for infant and 7.5 vs. 15 vs. 30 L/min for toddler; 2) Airvo2 set at 37°C and flows of 15 vs. 30 L/min for toddler; 3) large volume nebulizer (LVN) at flows of 1 vs. 2 L/min for infant and 1 vs. 2 vs. 4 L/min for toddler. Lastly, conventional nebulization was VMN with ultra via trach mask with O2 at 2 L/min and JN with T-piece attached to the airway for both models. The collected drug was eluted and assayed with ultraviolet spectrophotometry (276 nm).
Results:
Inhaled dose increased as the setting flows decreased for infant and toddler modes, regardless of the humidification devices (all P <.05) (Table 1). In-line placement of VMN with Optiflow and Airvo2 had a higher inhaled dose than LVN for toddler at all flow settings and for infant at moderate flow (all P < .05). Inhaled dose was higher with conventional VMN than in-line placement of VMN with humidification devices at all flow settings for both models tested (all P < .05). When conventional JN was utilized, the inhaled dose was higher than in-line placement of VMN with all humidification devices for toddler (all P < .05), except at low flow settings with Optiflow (13.9 ± 0.5 vs. 12.5 ± 1.3%, P = .016). In contrast, in-line VMN with Optiflow and LVN generated a higher inhaled dose than conventional JN at moderate flows for infant (both P < .05).
Conclusions:
During in-line placement of VMN with humidification devices, aerosol delivery increased as flow settings decreased, but the inhaled dose was lower than conventional VMN in both infant and toddler models. Nebulizer setups should be chosen based on patient oxygen and humidification needs.
Values are presented as mean ± SD, VMN: vibrating mesh nebulizer, JN: jet nebulizer, LVN: large volume nebulizer , a low flow settings were defined as 7.5 L/min with Optiflow and 1 L/min with LVN for toddler. b Moderate flow settings were defined as 5 L/min with Optiflow and 1 L/min with LVN for infant, and 15 L/min with Optiflow, 15 L/min with and Airvo2, and 2 L/min with LVN for toddler. c High flow settings were defined as 10 L/min with Optiflow and 2 L/min with LVN for infant, and 30 L/min with Optiflow, 30 L/min with and Airvo2, and 4 L/min with LVN for toddler.
Graphic representation of the study design View all access options for this article.Table 1. Percentage of the inhaled dose delivered through tracheostomy tube with different flow settings and humidification devices
Model
Nebulizer
Humidification device
Inhaled dose with flow settings, %
P value
Low flow a
Moderate flow b
High flow c
Infant
VMN
Optiflow
NA
5.0±0.4
0.7±0.1
.009
LVN
NA
3.8±0.2
2.5±0.5
.009
P value
.009
.009
VMN
None
22.8±3.3
JN
2.5±0.2
Toddler
VMN
Airvo2
NA
7.8±0.3
3.5±0.4
.009
Optiflow
13.9±0.5
7.7±0.6
3.9±0.8
.002
LVN
7.9±0.9
5.6±0.4
2.6±0.5
.002
P value
.009
.009
.045
VMN
None
23.1±1.9
JN
12.5±1.3
Get full access to this article