
Abstract
Background:
Accurate ETCO2 and PtcCO2 readings provide healthcare practitioners with data they need to determine the efficacy of medications, therapies, and the necessity of interventions. We tested the Procedural Oxygen Mask (POM) (POM Medical, Moorpark, California) to determine if there were differences between ETCO2 and PtcCO2 readings. We hypothesize there is no difference in ETCO2 and PtcCO2 readings on live participants while wearing the POM.
Methods:
First, a transcutaneous monitor (TCM) (Sentec, Lincoln, Rhode Island) was placed just below the left clavicle at the midclavicular line on each of the participants after prescreening and IRB approval. Then the POM was attached to a Medtronic Capnostream 35 ETCO2 Monitor (Medtronic, Minneapolis, Minnesota) and was placed on a participant’s face with medical air running through the mask at 10 L/min. After calibration, the PtcCO2 and the ETCO2 were recorded at 1 and 2 min. After 2 min, a Pentax Medical Video Bronchoscope VB-1530t2 (Pentax Medical, Montvale, New Jersey) was placed through the POM membrane. PtcCO2 and ETCO2 readings were measured at 1 and 2 min and the bronchoscope was removed. The participant then kept the mask on for 2 additional min and data were recorded. This process was repeated at flows of 12 and 15 L/min of medical air.
Results:
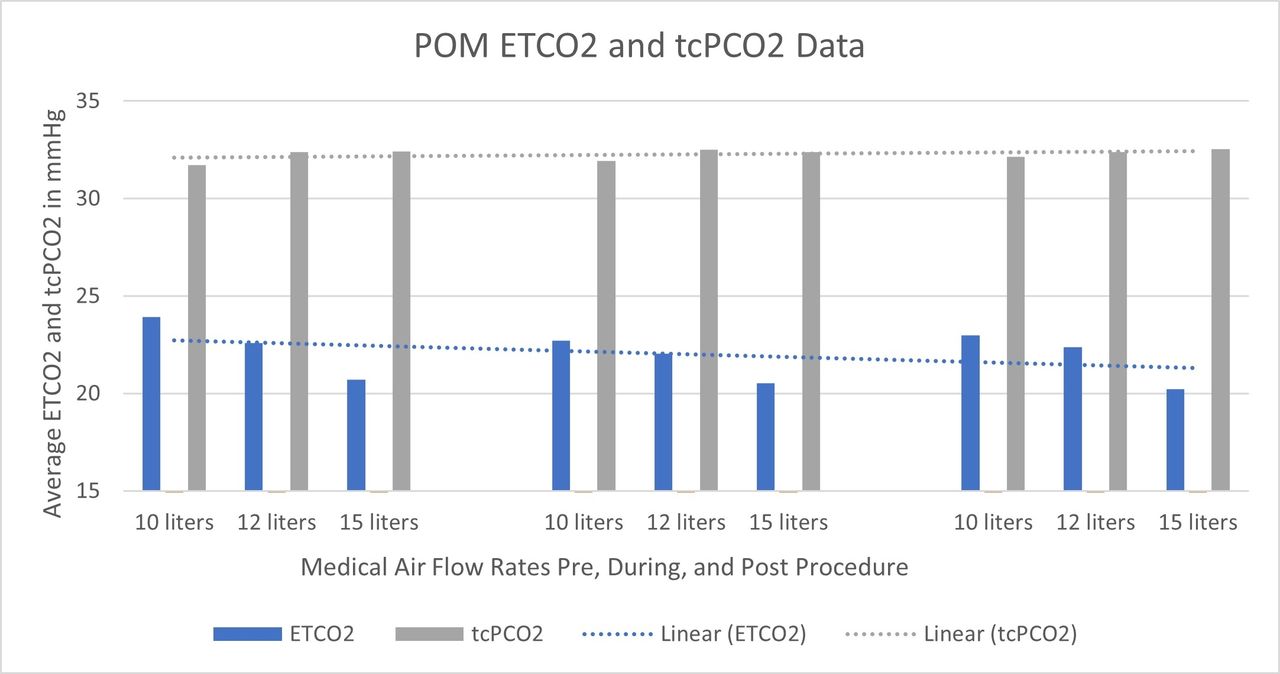
The average ETCO2 at 10, 12, and 15 L/min of air flow pre-procedurally was 23.93 mm Hg, 22.6 mm Hg, and 20.7 mm Hg. During the procedure at 10, 12, and 15 L the average ETCO2 was 22.73 mm Hg, 22.06 mm Hg, and 20.53 mm Hg. Post-procedurally, at 10, 12, and 15 L the average ETCO2 was 23 mm Hg, 22.37 mm Hg, and 20.23 mm Hg. See Figure 1. The average PtcCO2 at 10, 12, and 15 L of air flow pre-procedural was 31.73 mm Hg, 32.39 mm Hg, and 32.43 mm Hg. During the procedure at 10, 12, and 15 L, the average PtcCO2 was 31.93 mm Hg, 32.52 mm Hg, and 32.38 mm Hg. Post-procedural at 10, 12, and 15 L the average PtcCO2 was 32.16 mm Hg, 32.39 mm Hg, and 32.53 mm Hg. See Figure 1.
Conclusions:
It appears that with increases in flows via the POM, the measured ETCO2 decreases while PtcCO2 readings do not show much correlation with flows and less variance. Further research is required to determine if this is clinically significant. With these findings, the null hypothesis is rejected.
Get full access to this article
View all access options for this article.