
Abstract
Background:
Inhaled nitric oxide (iNO) delivered with a high-flow nasal cannula (HFNC) system is frequently utilized at our institution in children with congenital heart disease. An in vitro study of noninvasive iNO in a neonatal model identified differences between dialed and delivered iNO dose. Although the dialed iNO is known, the amount delivered to the trachea is unknown. Moreover, the effect of dialed iNO and HFNC flow on the amount delivered to the trachea is also unknown. The aim of this study was to evaluate iNO delivered dose at the tracheal level using a HFNC system in a spontaneously breathing pediatric model.
Methods:
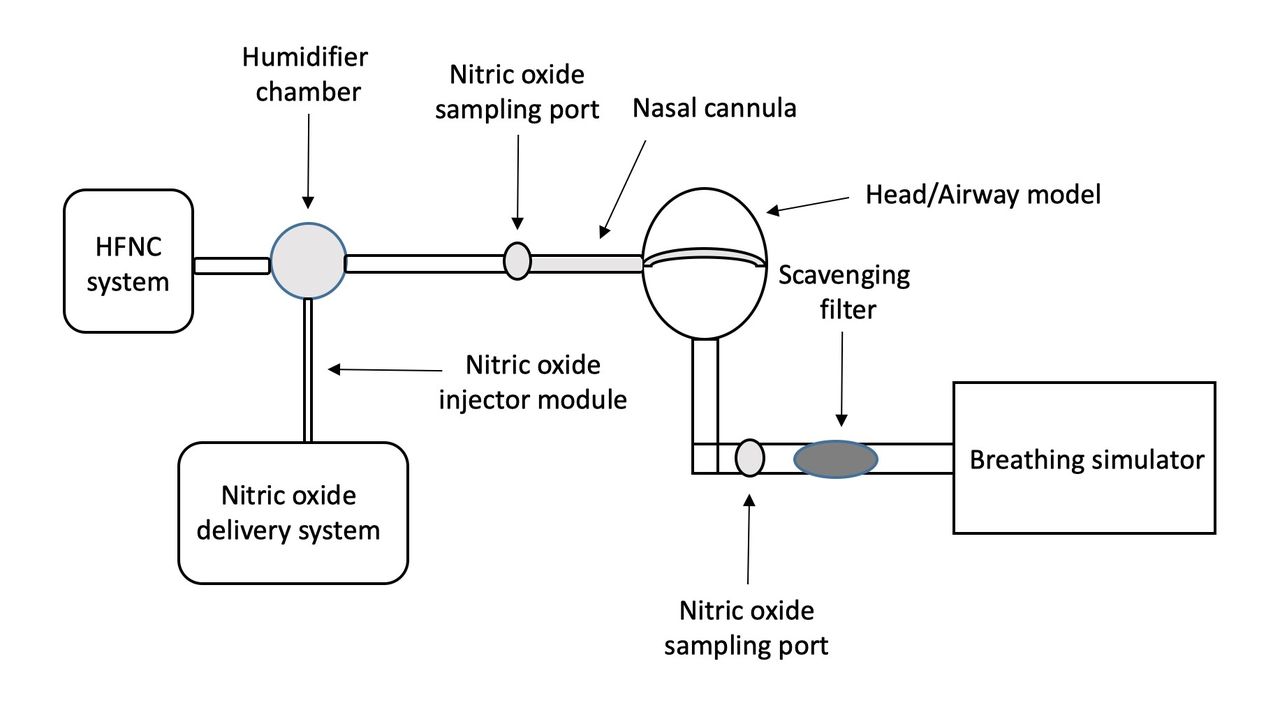
An anatomically correct 3D airway model of a 5-year-old child was connected in series to a scavenger filter and breathing simulator using normal and ARDS lung models (frequency 20 breaths/min, VT 125 mL, I:E 1:2, and frequency 30 breaths/min, VT 100 mL, I:E 1:1, respectively). An XL Optiflow Jr 2 nasal cannula (Fisher & Paykel) was used with flows 2, 3.5, 5, 7.5 10, and 25 L/min. The iNO delivery system (INOMax, Mallinckrodt) included an injector module placed at the humidifier chamber of the HFNC system (dry with heater off), a sampling line, and 2 sampling ports. One port was placed between the cannula and the circuit to monitor delivered iNO and the second was placed between the airway model and the scavenging filter to measure tracheal iNO concentrations. (Figure 1) The second port remained closed until the delivered iNO measurement was obtained. The sampling line was then switched to the second port and the first port was closed. Delivered and tracheal iNO measurements were recorded after 3 min for dialed concentrations of 5, 20, and 40 ppm. Experiments were performed in quadruplicate. Delta dialed iNO - delivered iNO, and tracheal iNO/dialed iNO (%) were calculated. General linear regression (lung model, dialed iNO, and flow) and descriptive statistics were performed.
Results:
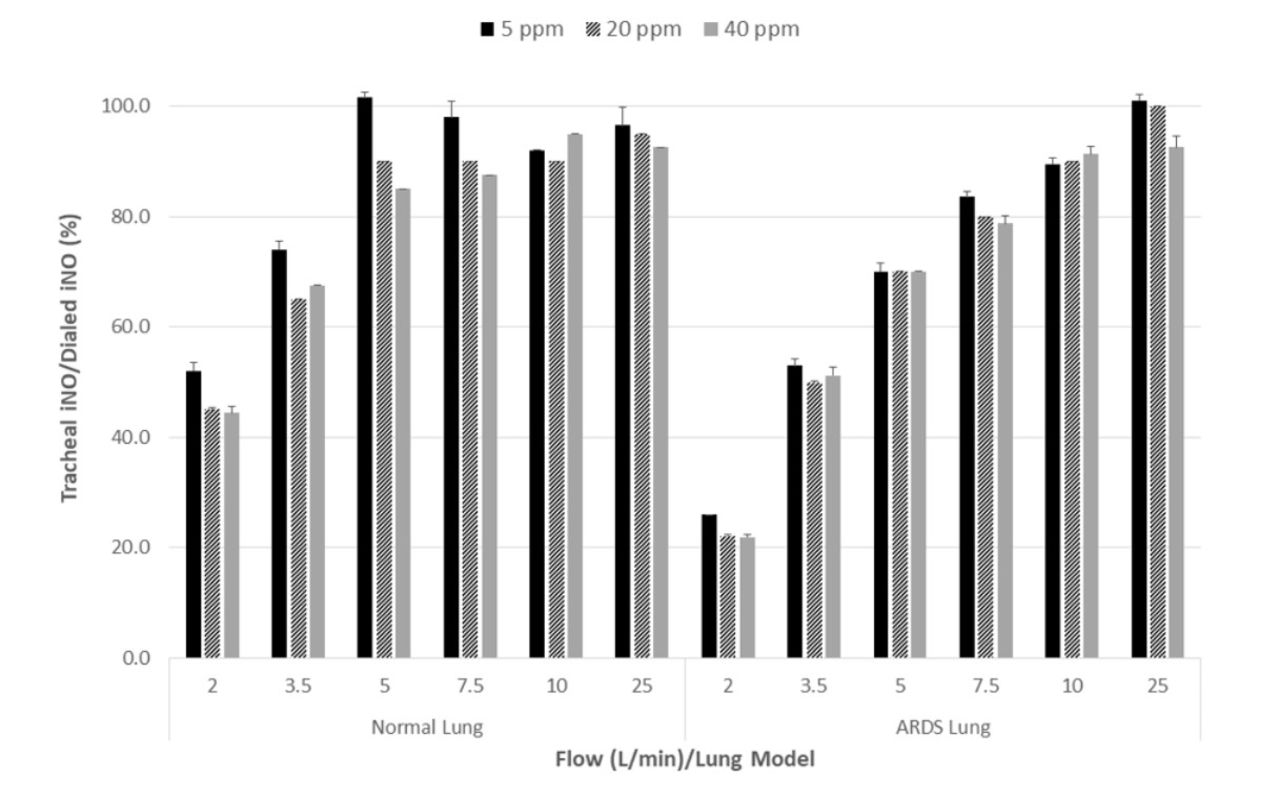
Median (IQR)/95%CI for delta (dialed - delivered iNO) and for tracheal/dialed iNO were 1 ppm (0-2 ppm)/0.4-2 ppm and 84.5% (56.8-92.4%)/76-90% (Figure 2). Linear regression analysis showed R2 of 0.49 (0.48 for the flow variable for flows 2-25 L/min) (P < .001) and R2 0.79 (0.67 for the flow variable for flows 2-10 L/min) (P < .001). The contribution of dialed iNO was minimal (R2 = 0.01).
Conclusions:
iNO was efficiently delivered to the trachea of a spontaneously breathing pediatric model using a nasal cannula and HFNC system (2-25 L/min). Efficiency was mainly affected by the flow but not by dialed iNO (5-40 ppm).
Get full access to this article
View all access options for this article.