
Abstract
Background:
Intrapulmonary percussive ventilation (IPV) facilitates airway clearance in small to mid-sized airways and promotes alveolar recruitment in diseases such as bronchiolitis, characterized by inflammation of lower airways, increased mucus production and increased airway resistance (Raw). However, in a recent adult model, excessive PIP was reported with IPV during instances of high Raw. The purpose of this study was to investigate pressure delivery between two IPV models in a simulated spontaneously breathing infant intubated for bronchiolitis.
Methods:
Six IPV devices, (3 IPV-1C and 3 IPV-2C, Percussionaire) using the same sliding venturi (Phasitron 5, Percussionaire) were connected to a lung simulator (ASL 5000, Ingmar Medical) via a 3.5 ETT and set to simulate a 5 kg 3 month old infant intubated for bronchiolitis (inspiratory and expiratory Raw of 142 and 158 cm H2O/L/s, respectively, CL of 4 mL/cm H2O, frequency 40 breaths/min, Ti 0.5, Pmus was set to achieve VT of 5 mL/kg). Settings based on previously published data of infants intubated for bronchiolitis. All IPV devices were tested at 30, 35, and 40 psi with frequency set at easy, mid, and hard. For the IPV-2C; demand valve, Ti, and inspiratory flow were set in 12 o’clock position. Tracheal (distal to ETT) and alveolar (distal to Raw) MAP and peak airway pressures (Paw) were obtained over four spontaneous breaths for each scenario. Values above 95th percentile were used to calculate Paw. Overall results for IPV models were based on average of each device (no. = 3). Descriptive statistics, T-test, and one-way ANOVA with Holm-Sidak were used for comparison between IPV models and intra-device variability.
Results:
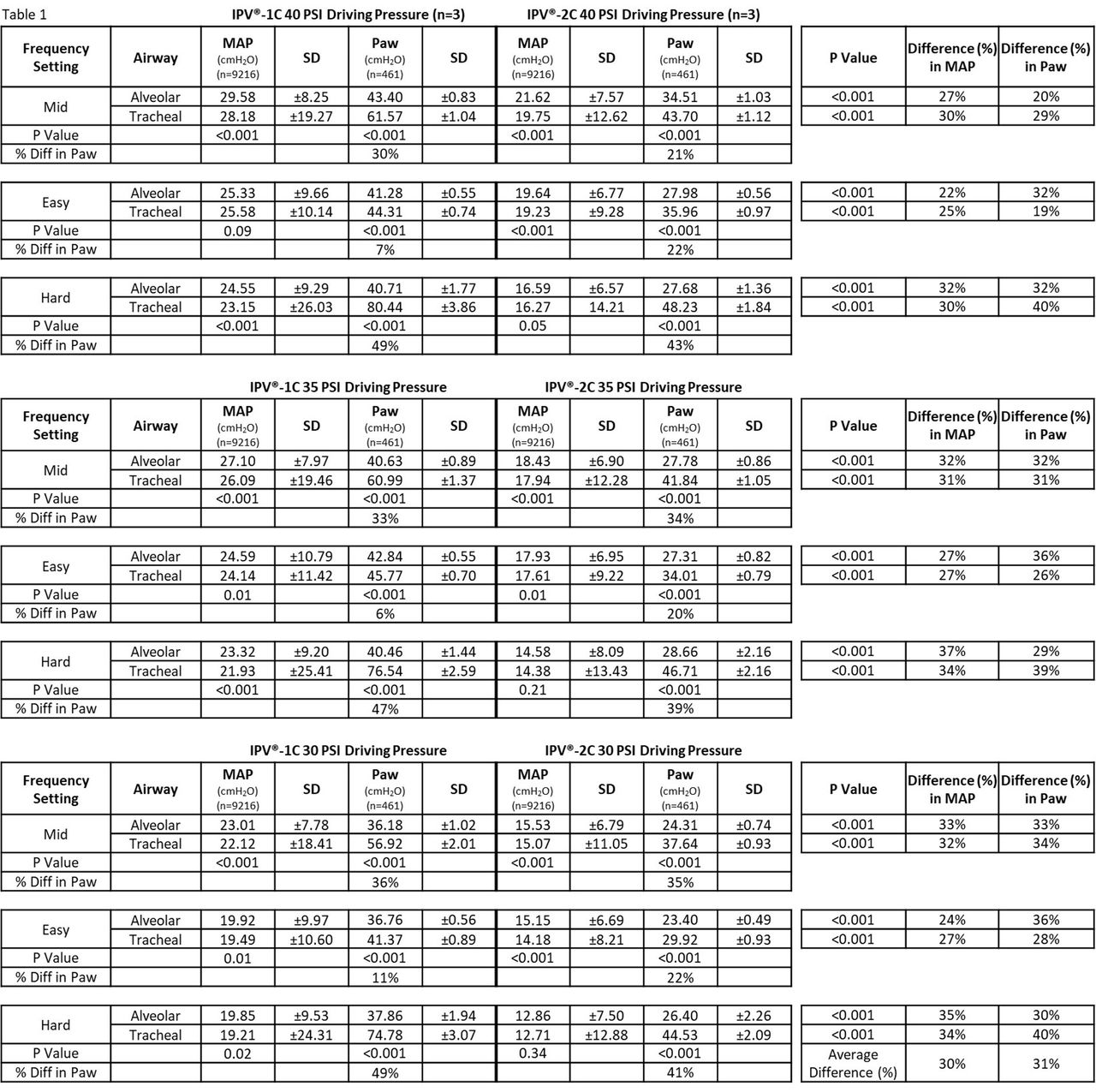
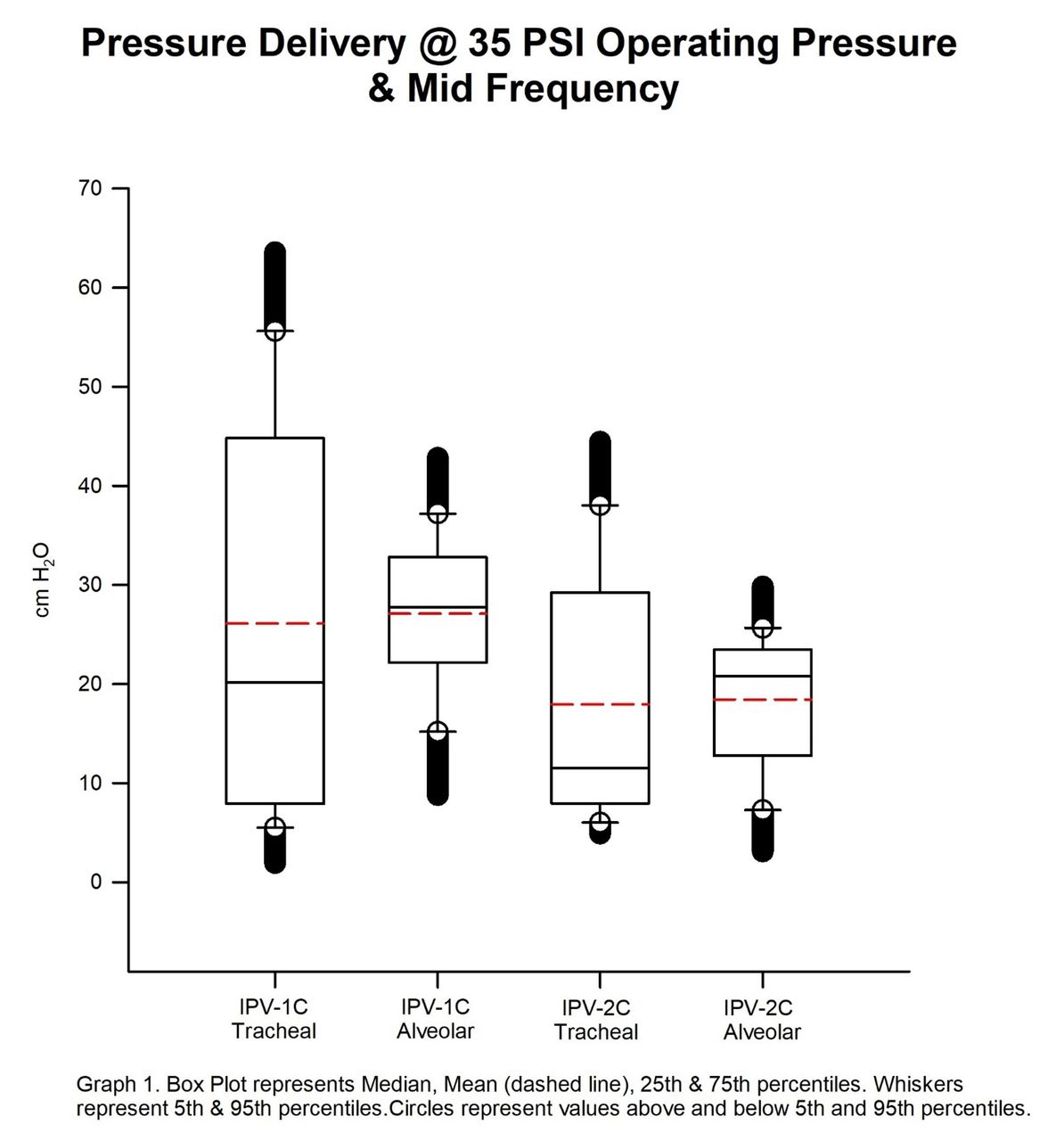
As shown in Table 1, the IPV-1C delivered significantly higher MAP (∼30%) and Paw (∼31%) in all tested scenarios compared to the IPV-2C (P < .001). Alveolar Paw was significantly less (P < .001) than tracheal Paw in all scenarios. The highest alveolar Paw value (43.40 cm H2O) was observed at 40 psi and mid setting with the IPV-1C. Significant intra-device variation was found in 25/27 comparisons with the IPV-1C, and 23/27 with the IPV-2C (P < .05).
Conclusions:
In this simulated infant model with high Raw, significant differences in pressure delivery were observed between IPV devices and models. While attenuation of tracheal to alveolar Paw was observed, clinicians should be aware of potentially elevated MAP and Paw when using operating pressures above 30 psi and/or at lower frequencies.
Get full access to this article
View all access options for this article.