
Abstract
Background:
Bag suction, a variant of manual hyperinflation, is frequently employed as a pulmonary hygiene technique in our pediatric intensive care unit (PICU). This practice involves scheduled disconnection from the ventilator, attaching a patient to a flow-inflating bag, manual ventilation, instilling normal saline, and suctioning the airway. Bag suction lacks standardized guidelines and uniform definitions, leading to variability. We undertook a quality improvement project aimed at evaluating the necessity and effectiveness of bag suction and examining the possibility of discontinuation.
Methods:
We conducted an audit of bag suction utilization at our institution, comparing its use to other pulmonary hygiene practices used in our PICU. We used workload tracking to gather metrics related to patients receiving invasive ventilation and bag suction, or other therapies. Stakeholders identified the reason for use, the most important components, and perceptions surrounding the practice. A survey composed of open and closed-ended questions, was disseminated to the PICU primary team and members of the PICU intensivist team. Education was implemented to reduce or eliminate bag suction in alignment with evidence-based recommendations derived from the audit and literature review. The findings were presented to stakeholder groups at several presentation sessions.
Results:
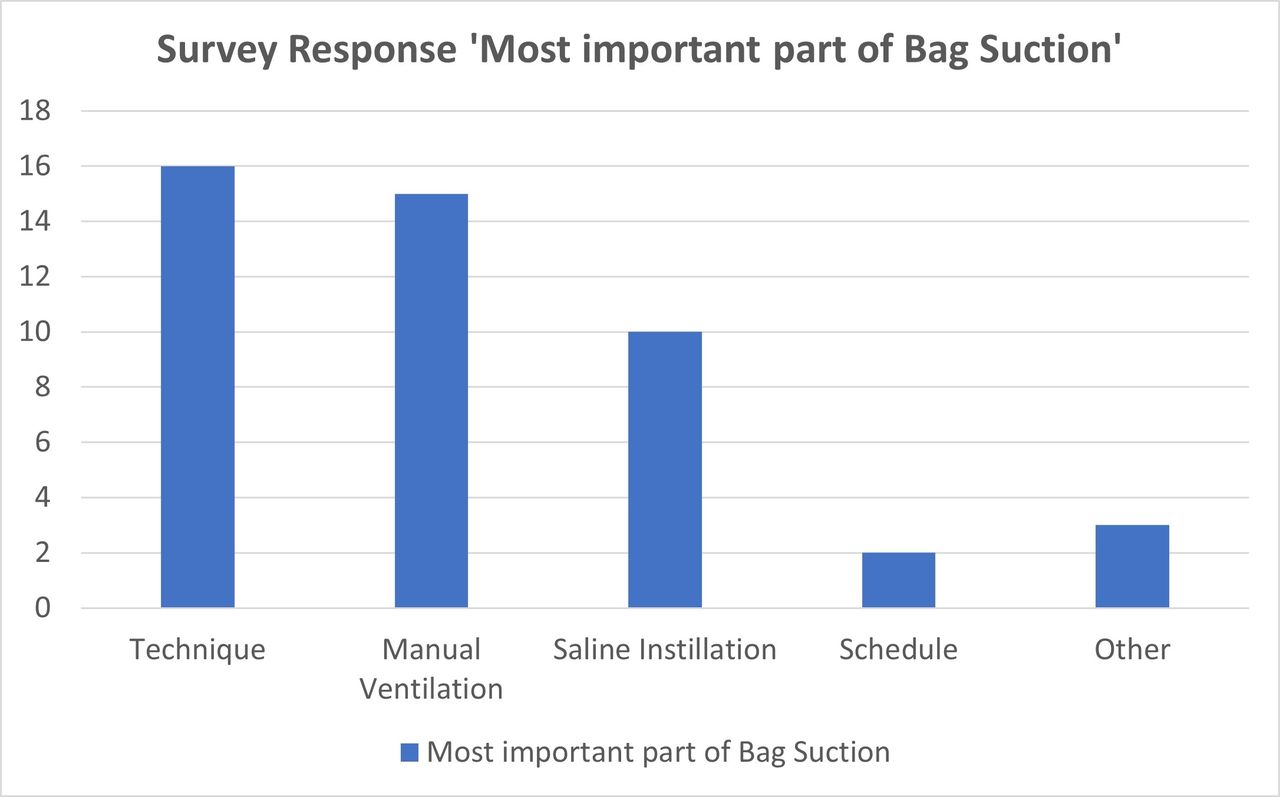
Stakeholder engagement demonstrated significant variation in reported perceptions, indications, goals, and methods. Consisting of 22 responses from respiratory therapists and physicians, the survey identified highly variable pressure targets. The audit revealed a high rate of bag suction utilization prior to education, with a reduction from an average of 29.3% for patients receiving invasive ventilation to an average of 9.9% following the presentation of our findings. After providing education, the decision was made to discontinue workload point allocation for this practice.
Conclusions:
Bag suction presents certain risks and does not show superiority over other available techniques. The use of a mechanical ventilator for lung expansion and minimizing saline instillation aligns more with evidence-based practice standards. Suction application should be driven by patient needs rather than a rigid schedule. The substantial reduction in bag suction following education interventions signals the potential for a phased-out discontinuation. This change necessitates sustained education and evidence-based policy adoption.
Mechanically Ventilated with Bag Suction orders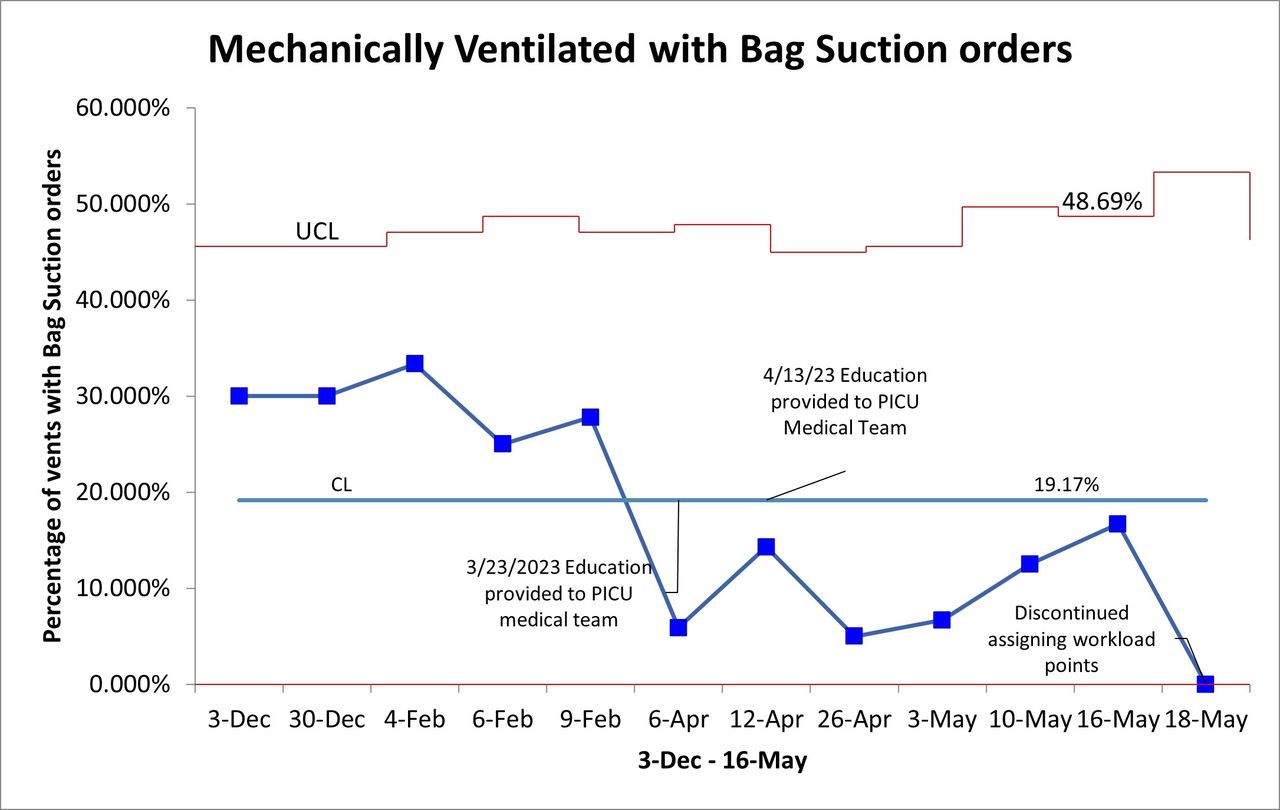
Get full access to this article
View all access options for this article.