
Abstract
Background:
Tracheostomy is a common procedure in critical care units. Many of those patients are breathing spontaneously and require nebulization to treat their underlying conditions. However, optimal aerosol delivery methods for these patients remain unclear. Thus, we aim to assess the impact of various factors on aerosol delivery, including nebulizer placements, flow settings, and interfaces, using vibrating mesh nebulizer (VMN) in-line with unheated humidification via large-volume nebulizer (LVN) for tracheostomized patients with spontaneous breathing, and compare it to conventional nebulization using jet nebulizer (JN) or VMN.
Methods:
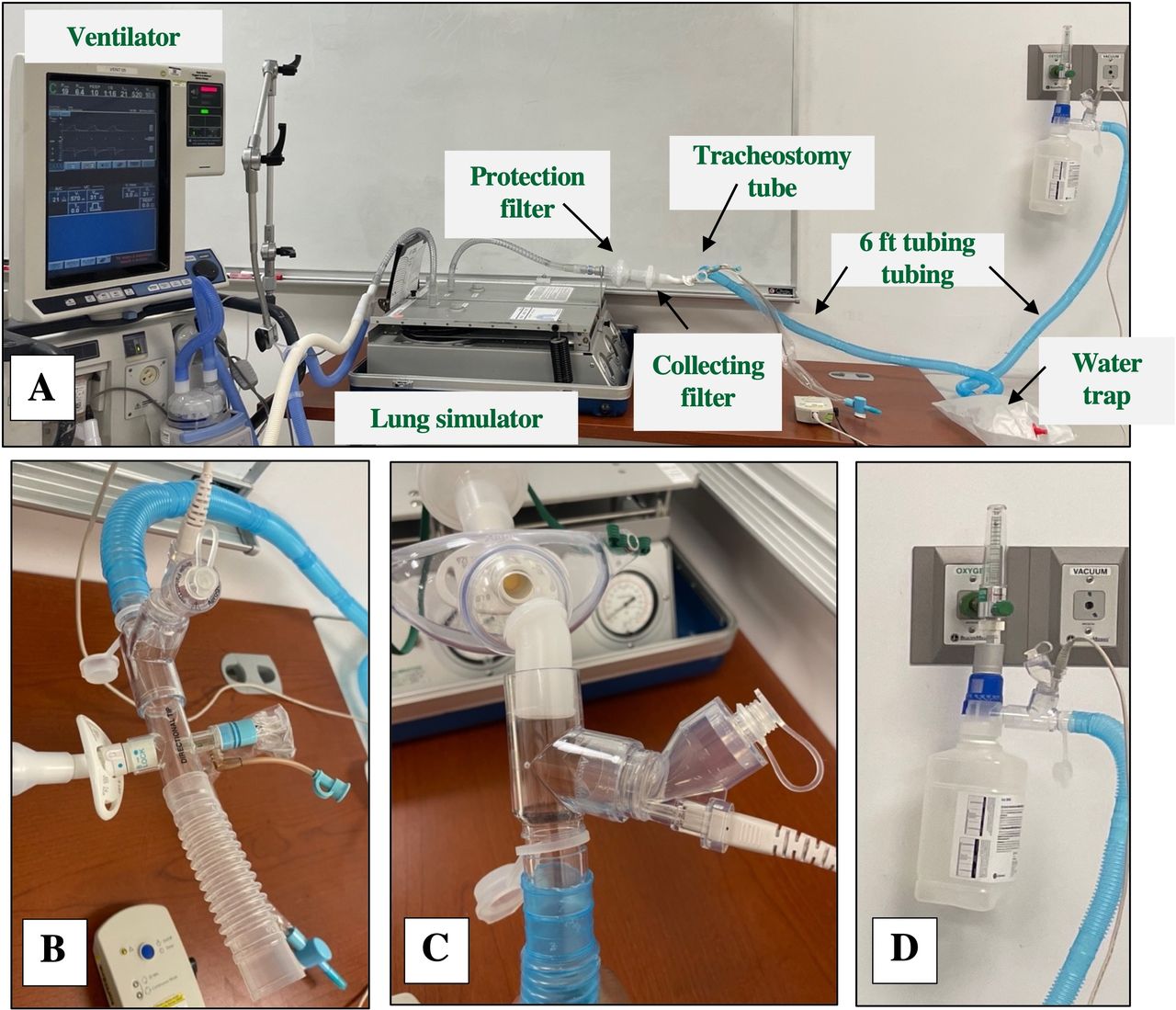
An adult tracheostomized spontaneous breathing model driven by a critical care ventilator was utilized, an 8.0 mm tracheostomy tube was connected to the lung model through a collecting filter. An Albuterol sulfate of 2.5mg/3mL was delivered via a VMN, which was placed in-line with LVN with FIO2 set at 0.28, in comparison to conventional nebulization using JN and VMN. The in-line aerosol delivery was compared at nebulizer placements of distal versus proximal to the lung model, using trach collar versus T-piece, and gas flows of 2 versus 6 L/min. Each condition was tested five times. The drug was eluted from the collecting filter and assayed with ultraviolet spectrophotometry (276 nm).
Results:
When VMN was placed in-line with LVN, the inhaled dose with the gas flow set at 2 L/min was 2-4 times higher than that with 6 L/min, regardless of the nebulizer placements and interfaces (all P < .01). The inhaled dose with VMN placed proximal to the lung model was higher than distal placement with both interfaces at 6 L/min (both P < .05), but lower at 2 L/min using tracheostomy collar (23.0 ± 1.6 vs 19.9 ± 1.1%, P = .016). Compared to the tracheostomy collar, T-piece had a higher inhaled dose at 6 L/min but a lower inhaled dose with VMN placed distal at 2 L/min (all P < .05). Regardless of the nebulizer placement and interfaces, the inhaled dose with VMN placed in-line with LVN at 2 L/min was comparable to that with conventional nebulization using VMN but higher than JN.
Conclusions:
Aerosol delivery via the in-line placement of VMN with an LVN was significantly affected by nebulizer placement, interface, and gas flow settings. The inhaled dose increased as the flow decreased. At low gas flow settings (2 L/min), the inhaled dose was similar to that with conventional nebulization using VMN and tracheostomy collar.
Values are presented as mean ± SD, Significant difference (P < .05), LVN: large volume nebulizer, VMN: vibrating mesh nebulizer, JN: jet nebulizer
A) Study set-up, B) Proximal in-line placement with T-piece, C) Proximal in-line placement with tracheostomy collar, D) Distal in-line placement. View all access options for this article.Percentage of inhaled dose delivered through tracheostomy tube with proximal and distal nebulizer positions in various conditions
Set-up
Nebulizer
Interface
Flow (L/min)
Inhaled dose at the proximal placement
Inhaled dose at distal placement
P value
In-line with LVN
VMN
T-piece
6
9.4 ± 0.2
7.1 ± 0.3
.009
2
20.2 ± 0.9
19.6 ± 0.8
.675
P value
.009
.009
Trach collar
6
5.6 ± 0.6
4.7 ± 0.3
.028
2
19.9 ± 1.1
23.0 ± 1.6
.016
P value
.009
.009
Conventional
VMN
Trach collar
2
21.9 ± 1.6
JN
Trach collar
8
14.2 ± 0.8
T-piece
12.5 ± 0.2
Get full access to this article