
Abstract
Background:
Elderly patients often have poor inhaler technique, resulting in ineffective deposition of medication in the lungs. Low motivation, a short attention span, and poor medication adherence pose substantial challenges for health educators when teaching inhaler techniques. Regarding a solution to these challenges, this study compared the effectiveness of a traditional training method with that of a tailored training program in enhancing the inhaler technique of elderly inpatients in Taiwan.
Methods:
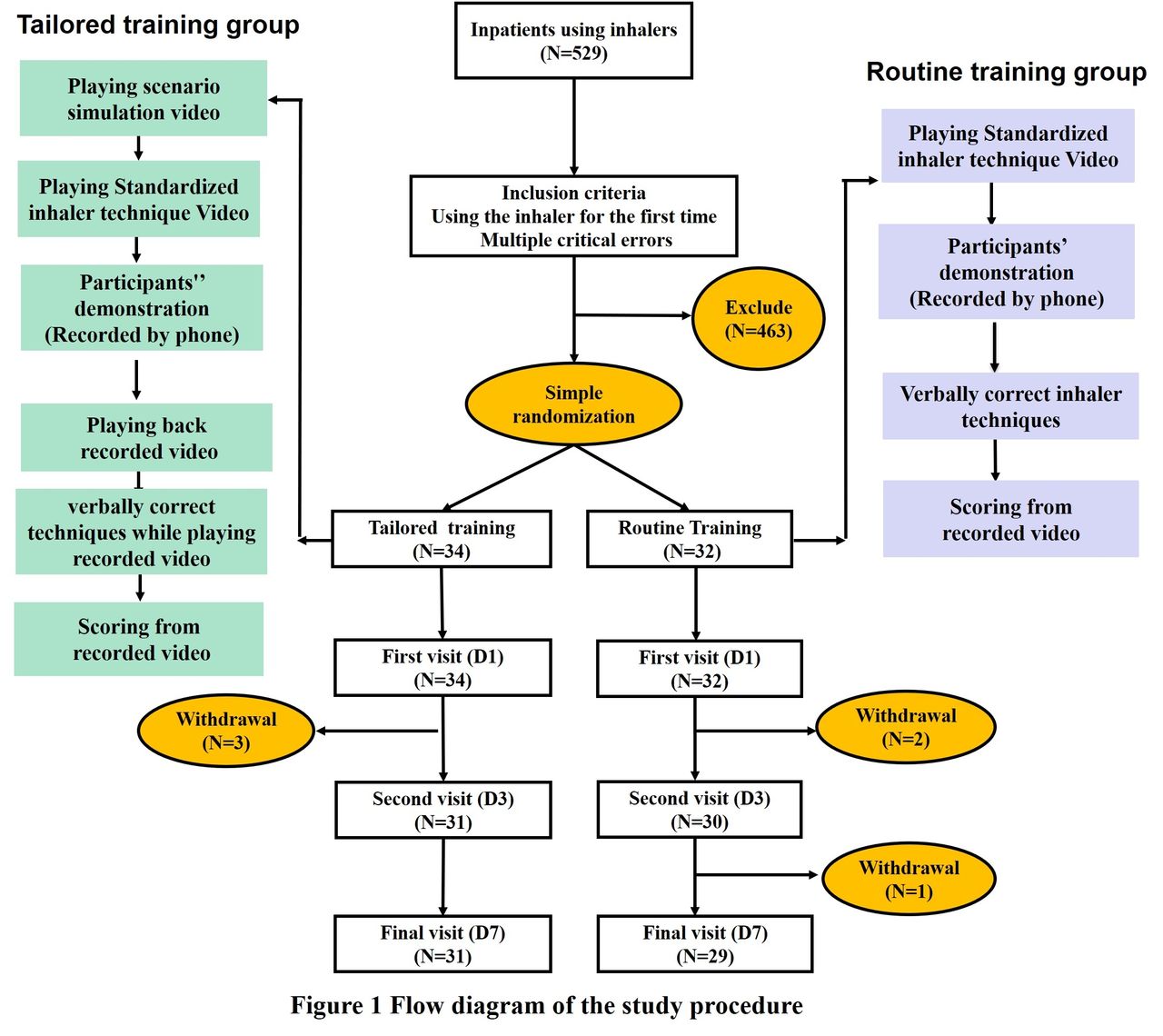
Participants were randomly assigned to the tailored training group (TG) or routine training group (RG). The TG received three-step training involving scenario simulation videos, a standardized guiding video, and verbal corrections after the recorded videos (patient demonstration) had been played. The RG group received only verbal corrections from a respiratory therapist following self-demonstration after watching the inhaler guiding video. Inhaler technique was assessed by reviewing the videos recorded on days 1, 3, and 7. Data were analyzed using JASP, with descriptive statistics for patient characteristics. An independent-samples t test was used to compare critical error ratios, with statistical significance set at P < .05.The study was approved by the Institutional Review Board of Chang Gung Medical Foundation (approval no.202001107B0) and the procedures of this study adhered to the Declaration of Helsinki.
Results:
Achieving adequate inhalation was a challenging process; the success rate was 58.0% and 51.7% in the TG and RG, respectively. Analysis of the learning effect revealed a significant intergroup difference on day 7. The proportion of participants with critical inhaler technique errors was significantly lower in the TG group (TG = 0.42 ± 0.50, RG = 0.69 ± 0.47, P = .03).
Conclusions:
Compared with traditional methods, the proposed tailored training program was considerably more effective in improving the inhaler technique of elderly inpatients. Scenario simulations enhance patients’ understanding of asthma and chronic obstructive pulmonary disease resulting from inhaler misuse. Video observation also aids in rectifying errors and overcoming reluctance to acknowledge mistakes. These findings can serve as a reference educational model for healthcare providers in hospitals. However, studies on a larger scale are required.
TG: tailored training group; RG: routine training group; COPD: chronic obstructive pulmonary disease; p < 0.05*.
View all access options for this article.Patient characteristics
TG(n=31)
RG(n=29)
p
Age
70.19 ± 10.89
69.60 ± 10.72
0.916
Gender (male)
25 (80.6%)
23 (79.3%)
0.305
COPD
2 (6.5%)
2 (6.9%)
0.946
Asthma
1 (3.2%)
4 (13.8%)
0.144
Coronary artery disease
5 (16.1%)
3 (10.3%)
0.518
Diabetes mellitus
7 (22.6%)
4 (13.8%)
0.388
Hypertension
8 (25.8%)
6 (20.7%)
0.646
Lung cancer
7 (22.6%)
5 (17.2%)
0.613
Chronic kidney disease
3 (9.7%)
2 (6.9%)
0.946
No disease history
10 (32.6%)
9 (31.0%)
0.144
Active smoker
15 (48.4%)
13 (44.8%)
0.787
Living with a caregiver
24 (77.4%)
24 (82.8%)
0.613
Educational level below elementary school
23 (74.2%)
19 (65.6%)
0.472
Inhaler Technique Checklist: Day 7
TG(n=31)
RG(n=29)
Correctly opening the canister
31 (100%)
29 (100%)
Correctly administering the medication
31 (100%)
29 (100%)
Correctly filling the medication
31 (100%)
29 (100%)
Correctly sealing the inhaler mouthpiece
29 (93.5%)
26 (89.7%)
Correctly exhaling completely before inhaling
24 (77.4%)
19 (65.5%)
Correctly inhaling with an adequate flow rate
18 (58.0%)
15 (51.7%)
Correct hand–mouth coordination
21 (67.7%)
22 (75.9%)
Correctly holding breath
28 (90.3%)
22 (75.9%)
Correctly confirming the remaining dose
30 (96.8%)
28 (96.6%)
Proportion of participants making a critical error
TG(n=31)
RG(n=29)
p
First visit (day 1)
0.87 ± 0.34
0.90 ± 0.31
0.76
Second visit (day 3)
0.58 ± 0.50
0.72 ± 0.46
0.25
Final visit (day 7)
0.42 ± 0.50
0.69 ± 0.47
0.03*
Get full access to this article