
Abstract
Background:
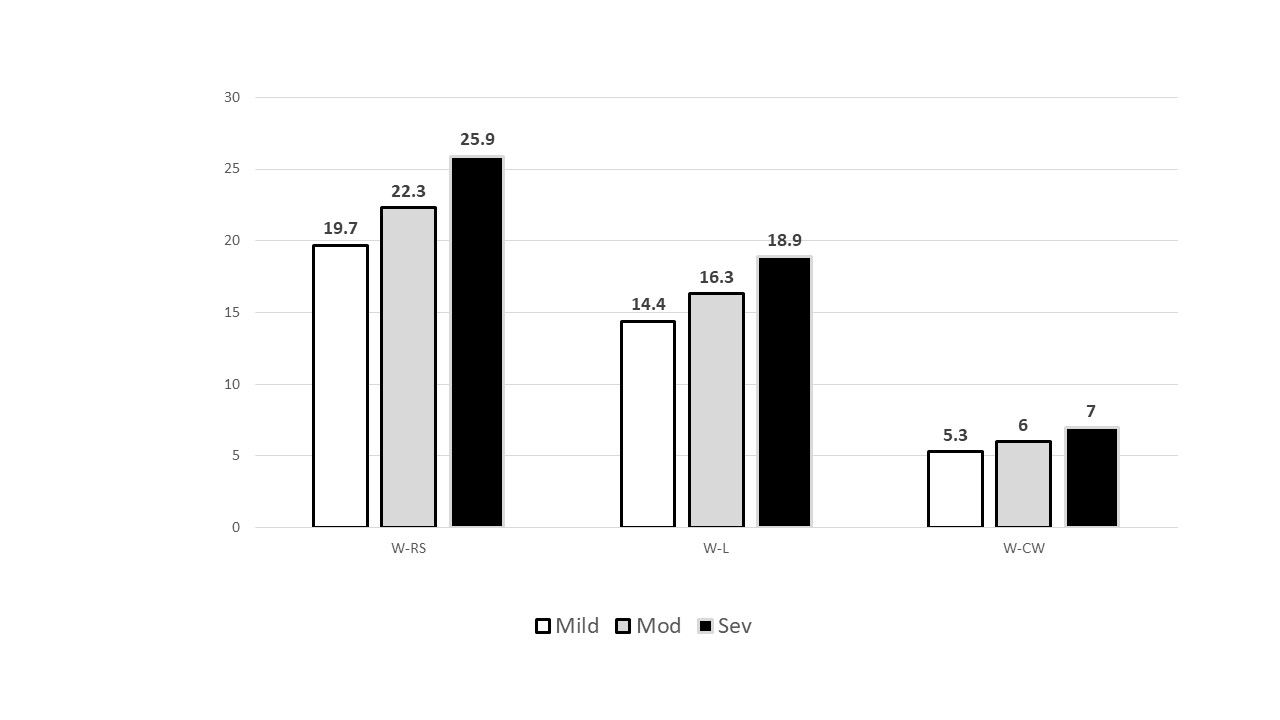
Mechanical power transferred to the lungs and chest wall (ie, WRS) over time (J/min) is linked to both ventilator-induced lung injury and ARDS mortality. Berlin definition ARDS-related mortality increases from mild (27%), to moderate (32%), to severe (45%)1 with relative increases of 119% and 167% respectively. This retrospective study examined whether WRS intensity also increases across Berlin demarcations, and if it approximates that of the corresponding mortality rise.
Methods:
948 ARDS subjects were studied who: 1) met the Berlin definition, 2) were managed with ARDSNet protocols initiated ≤ 24 h after ARDS onset, and 3) survived ≥ 24 h after protocol initiation (allowing lung-protective ventilation optimization and censoring moribund cases). A simplified WRS calculation (0.098 x frequency x VT x [PEEP + PDR]),2 was used whereby WL and WCW were estimated using fractional subcomponents respiratory system elastance: EL/ERS (0.72), ECW/ERS (0.28).3 Data were analyzed using the Kruskall-Wallis test and Dunn’s post-test. Alpha was set at 0.05.
Results:
With one exception (WCW: mild vs. moderate) all measures of W transfer increased significantly: moderate vs. mild (P = .019), severe vs. moderate (P < .001) and severe vs. mild (P < .001). The proportional increase in W transfer increased by 113% between mild and moderate ARDS, 116% between moderate and severe ARDS and 131% between mild and severe ARDS.
Conclusions:
Estimated median WRS transferred from the ventilator to the respiratory system and its lung and chest wall subcomponents increased steadily as ARDS severity increased from mild to moderate to severe acute lung injury, however it occurred at a rate substantially below that of mortality rise. 1. Berlin Taskforce. JAMA 2012;307:2526. 2. Chiumello D et al. Crit Care 2020;24:417. 3. Kallet RH et al. Respir Care 2007; 52(8):989.
Get full access to this article
View all access options for this article.