
Abstract
Background:
Optimum mechanical ventilation requires determining which goal is most important (ie, safety, comfort, or liberation) and selecting a mode that best serves the goal. Ongoing adjustment of settings is then required. For liberation, a switch must be made from mandatory to spontaneous breaths, usually done manually. Staffing shortages and the increasing number of ventilated patients can delay needed mode changes and adversely affect patient outcomes. Automode, a feature included on Getinge Servo-I and Servo-U ventilators, automatically switches between mandatory and spontaneous breaths. Spontaneous breaths suppress mandatory breaths until an apnea occurs. The period from the last spontaneous breath to the reappearance of the first mandatory breath is determined by a calculated apnea time limit (ATL) which is based, in part, on a maximum apnea time (MAT) setting (7-12 s). However, unlike apnea settings on other modes, ATL is automatically adjusted based on the MAT setting, the mandatory breath rate setting (MBR) and the spontaneous breath count (SBC) since the last mandatory breath. This functionality is unusual and not explained clearly in the operator’s manual. Therefore, the purpose of this study was to describe and validate the (ATL) algorithm using simulated mechanical ventilation.
Methods:
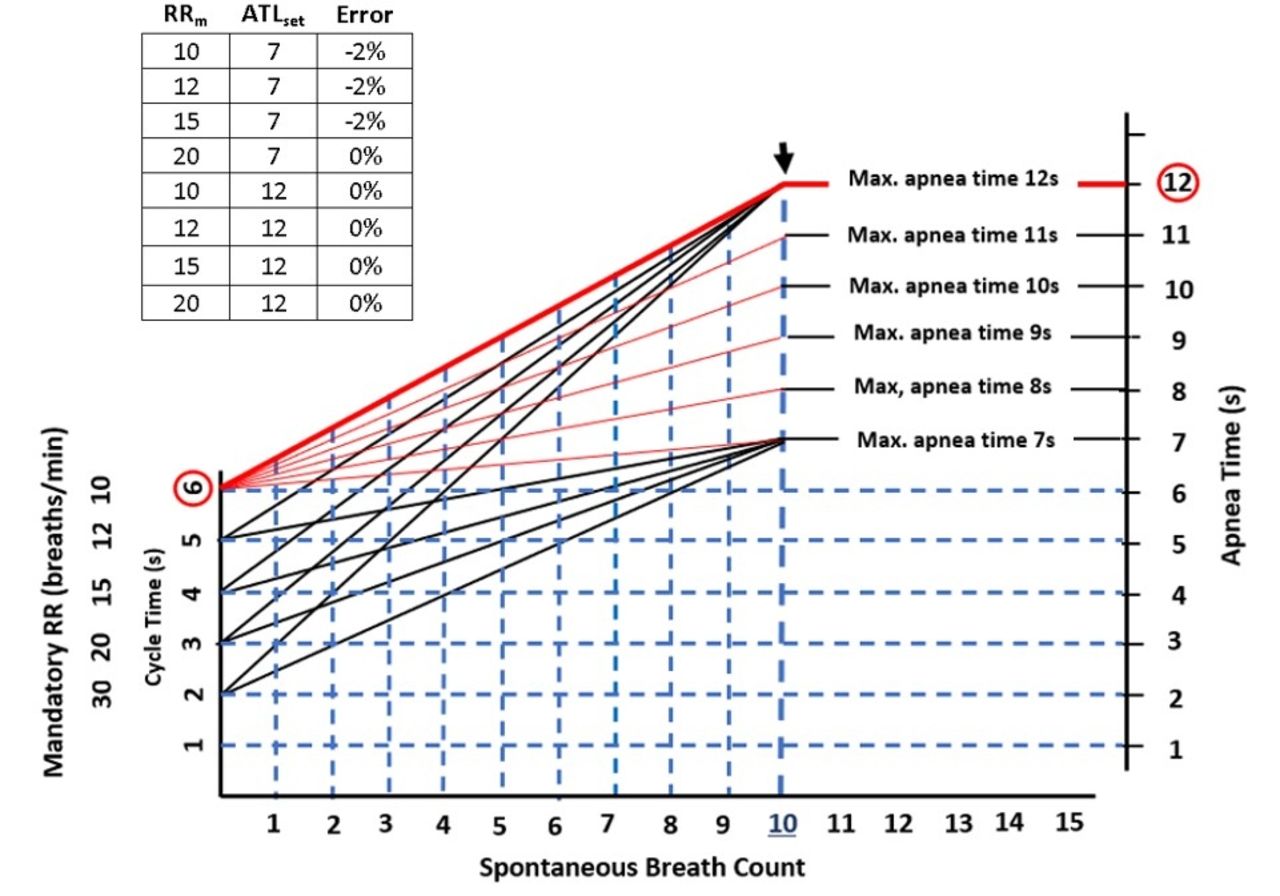
A SERVO-U ventilator was connected to an ASL 5000 breathing simulator (IngMar Medical). Ventilator settings: Automode (Pressure Control to Pressure Support), PC = 10 cm H2O, PS = 5 cm H2O, PEEP = 10 cm H2O, MBR = 10, 12, 15, 20 breaths/min. MAT = 7 and 12 s. Simulator settings: resistance = 10 cm H2O/L/s, compliance = 35 mL/cm H2O, Simple Flow Trigger Model: rate = 20 breaths/min, trigger flow = 10 L/min, trigger duration = 800 ms. Script: SBC = 0-12 breaths. Flow waveforms were recorded and observed ATL was compared to the calculated ATL. Equation provided by Getinge: calculated ATL = (60/MBR) + (SBC × (MAT - (60/MBR))/10). The outcome variable was error (%) = 100% × (observed ATL – calculated ATL)/calculated ATL, averaged across the SBC range.
Results:
The graph shows expected performance according to equation (red is max ATL). The observed ATL for MAT = 7s ranged from 3s (MBR = 20, SBC = 0) to 7s (MBR = 10-20, SBC = 10-12). The observed ATL for MAT = 12s ranged from 3s (MBR = 20, SBC = 0) to 12s (MBR = 10-20, SBC = 10-12). Average error ranged from 0 to –2%.
Conclusions:
The performance of the apnea time limit feature was as expected.
Get full access to this article
View all access options for this article.