
Abstract
Background:
High-velocity nasal insufflation (HVNI) is a form of oxygen therapy and respiratory support that provides flows higher than traditional oxygen delivery devices. In the last decade, a proliferation of high flow nasal cannula devices and dosing capabilities have been introduced into the clinical setting without evidence of appropriate dosing in L/min/kg recommendations. HVNI facilitates a well-described mechanism of improving ventilatory efficiency by way of eliminating carbon dioxide traditionally stacked in anatomical dead space of the upper airway, therapeutic humidification, and low levels of positive airway pressure.
Methods:
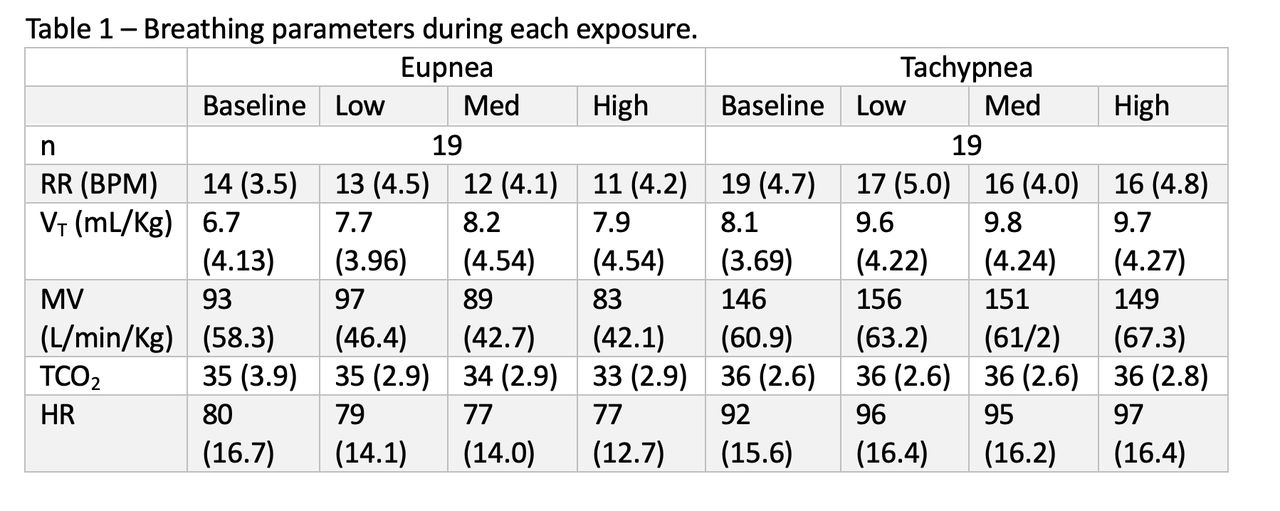
Following IRB approval, a prospective, randomized intra-patient trial of three different HVNI flows (0.2 Low, 0.3 Med and 0.4 High L/kg/min PBW) at 0.21 FIO2 were used to evaluate ventilation efficiency of healthy subjects. Measurements of minute ventilation (VE), respiratory rate (RR) and tidal volume (VT) were used during two model of breathing (eupnea and tachypnea). Transcutaneous CO2 was used to standardize VE (mL/kg) to a CO2 of 40 mm Hg. Baseline (without HVNI) recordings of eupnea and tachypnea were used as a comparison of the influence of HVNI.
Results:
20 healthy subjects were enrolled with an average age of 26 (± 12.3) years of age of whom 65% were male. 19 subjects were analyzed, due to an export error of one subject’s data. MV was not found to be statically different from baseline. RR was found to be significantly lower, and VT was significantly higher with the use of HVNI than baseline in both models.
Conclusions:
HVNI improves respiratory efficiency by increasing VT and triggering a lower RR response to maintain a consistent VE regardless of breathing model. These results do not support that efficiency gained from HVNI was from dead space washout at the levels used in this study.
Get full access to this article
View all access options for this article.