
Abstract
Background:
Best practice for asthma management is driven by two major guidelines: the Global Initiative for Asthma Management (GINA) and the National Heart, Lung, and Blood Institute Expert Panel Report 3. Both guidelines recommend provision of asthma education at every encounter and measuring spirometry at diagnosis/start of asthma treatment, 3-6 months after starting controller treatment, then periodically. Orders for a written asthma action plan (AAP) with education and spirometry are at the discretion of a licensed independent practitioner at our institution. An initial chart review revealed that AAPs and spirometry were not consistently ordered in the primary care clinics. This quality improvement study aimed to increase frequency of ordered spirometry and AAPs in children with asthma seen in primary care through use of a respiratory therapist (RT)-driven protocol.
Methods:
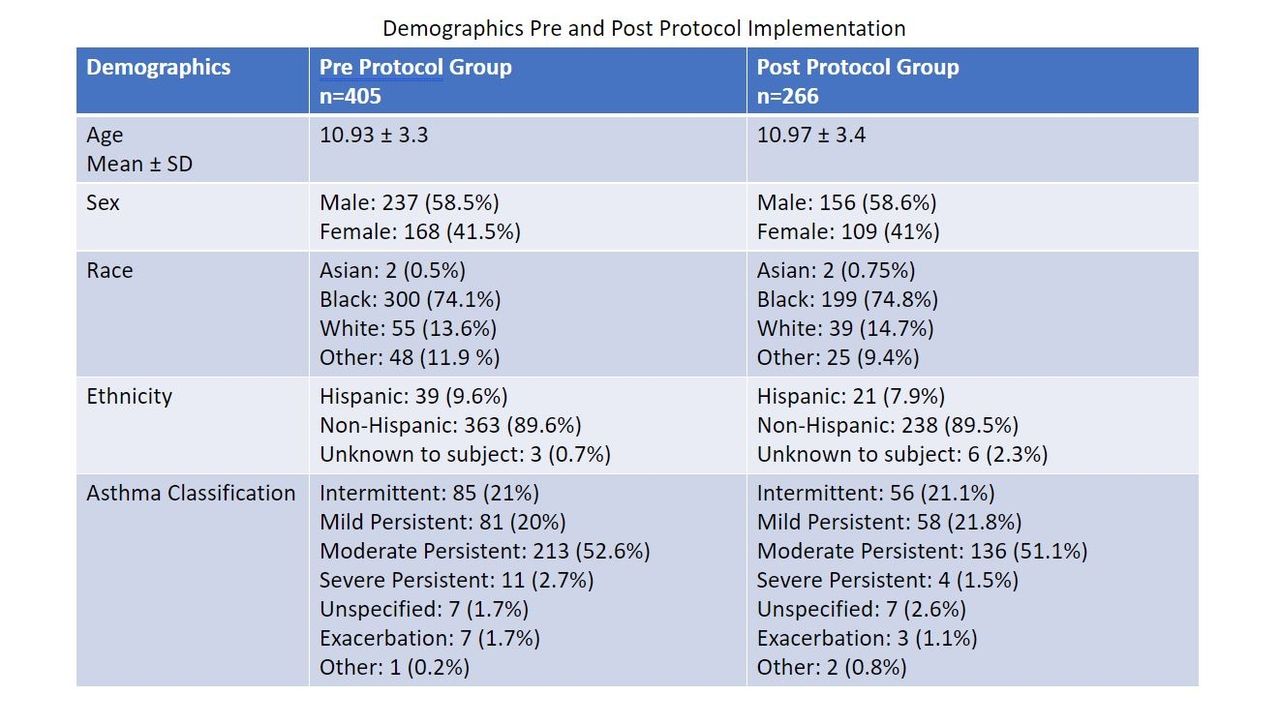
Children with asthma ≥ 6 years of age scheduled for a primary care asthma-specific exam or health supervision exam were included. The protocol established that spirometry and AAPs were to be done annually for intermittent asthma and every 6 months for persistent asthma. The RTs identified eligible subjects and placed the electronic medical record orders one day before the clinic visit. Six months of data were collected before implementation of the protocol. Data included: subject demographics, asthma severity classification, reason for visit, and if spirometry and/or AAP were ordered during the visit. A SMART goal was established to increase the percentage of appropriate spirometry and AAPs completed to ≥ 80% over a 6-month period. Proportions before and after the implementation were compared with Chi-square statistics
Results:
Prior to protocol implementation, spirometry and AAP were completed in 68.2% (236/346) and 63.8% (229/359) of eligible children respectively. Following protocol implementation, spirometry and AAP were completed in 93.4% (228/244) and 87.2% (204/234) of eligible children respectively (P < .001 for both outcomes).
Conclusions:
Utilization of spirometry and AAPs in asthmatic children seen in an outpatient primary care setting significantly increased after the implantation of an RT-driven protocol.

Get full access to this article
View all access options for this article.