
Abstract
Background:
Atelectasis results when alveoli collapse and is prevalent in approximately 90% of patients undergoing periods of sedation and mechanical ventilation (MV). The pathophysiological effects of atelectasis include decreased lung compliance and decreased gas exchange capacity, leading to lung injury. Current strategies to minimize atelectasis are centered around an ‘open lung’ approach that relies on PEEP to maximize alveolar patency. Our research investigates the use of temporary transvenous diaphragm neurostimulation (TTDN) to provide controlled diaphragm contractions during mechanically ventilated breaths to maximize alveolar patency. Compliance is a measure of the elastic resistance of a system and correlates with the number of patent alveoli. Changes in lung compliance reflect elastic changes in lung tissue and affect the amount of mechanical work required to support the patient with positive-pressure ventilation. Reduced lung compliance reflects pathological change and indicates potential risk for ventilator-induced lung injury (VILI) in sedated patients.
Methods:
A study was conducted using 50-60 kg pigs, mechanically ventilated for 12 hours after oleic acid-induced lung injury, a preclinical model of ARDS. The MV group received lung-protective volume control ventilation at 8 mL/kg (6 animals). The MV+TTDN100% group also received TTDN on every breath in synchrony with the inspiratory phase of volume control ventilation. The strength of diaphragm contraction targeted a reduction in ventilator pressure-time product of 15-20% during inspiration (6 animals) as previously published. Static lung compliance was measured by esophageal pressure manometry using a respiratory monitor. Measurements were taken at baseline, after achievement of lung injury, and 12 hours post-injury. Data is reported as median with interquartile ranges, and Mann-Whitney U-test was used for statistical analysis.
Results:
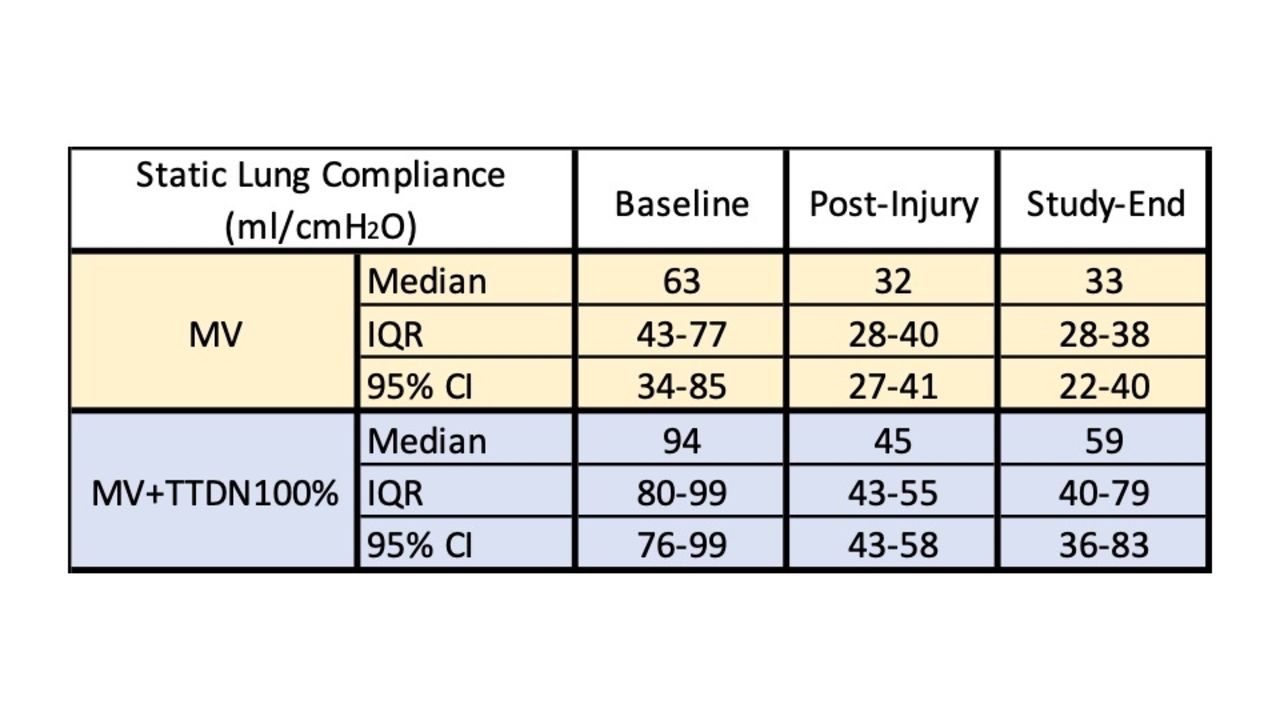
Static lung compliance was 49% higher at baseline, 41% higher after oleic acid-induced lung injury, and 79% higher at study-end in the MV+TTDN100% group. Refer to Table 1 and Figure 1.
Conclusions:
Negative-pressure-assisted ventilation, comprised of transvenous diaphragm neurostimulation during inspiration combined with volume control mechanical ventilation, improves static lung compliance at all study points in a preclinical model of ARDS. TTDN has the potential to improve outcomes by reducing VILI if these results translate into human ARDS patients.
Figure 1: Median (IQR) Static Lung Compliance Table 1.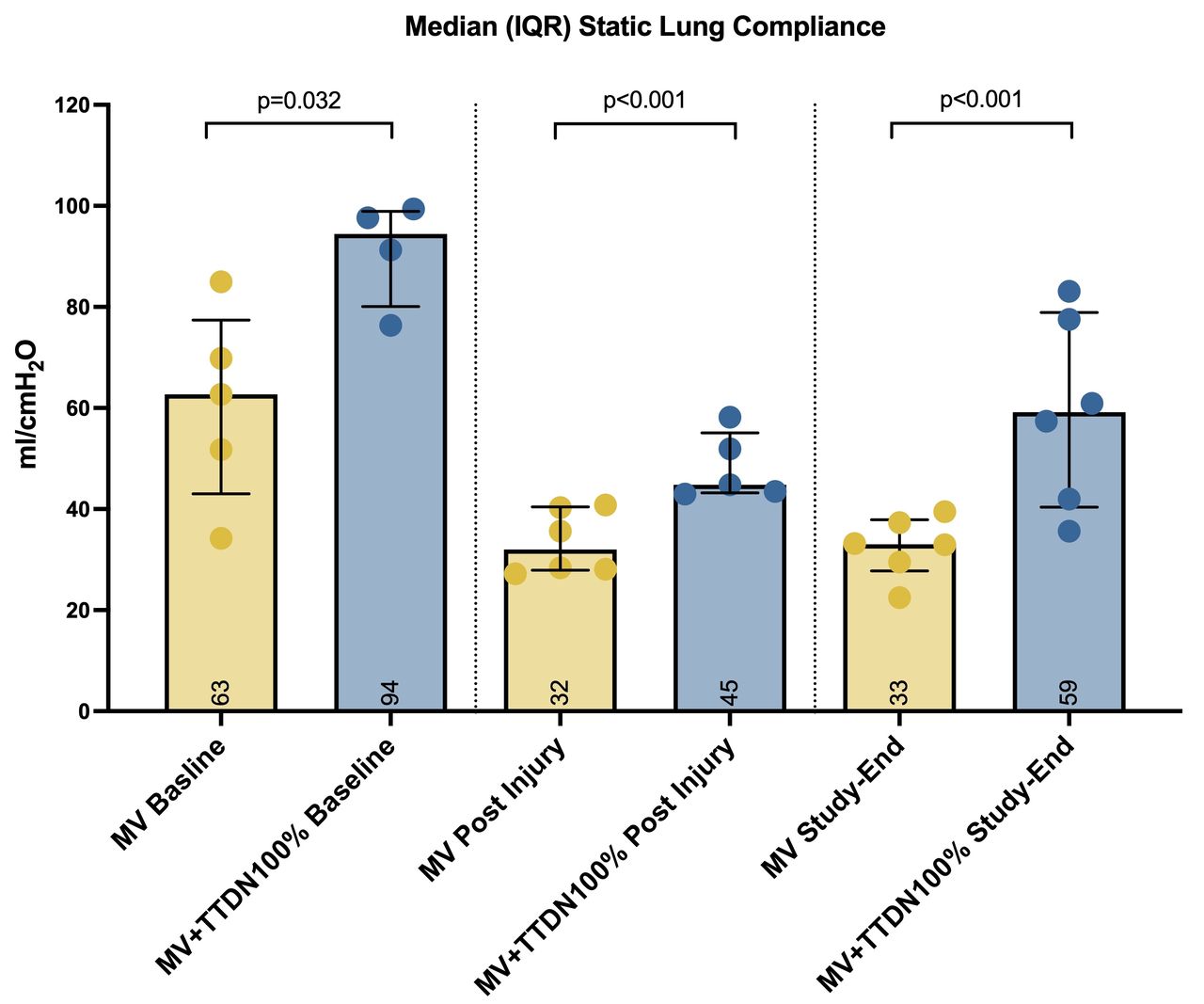
Get full access to this article
View all access options for this article.