
Abstract
Background:
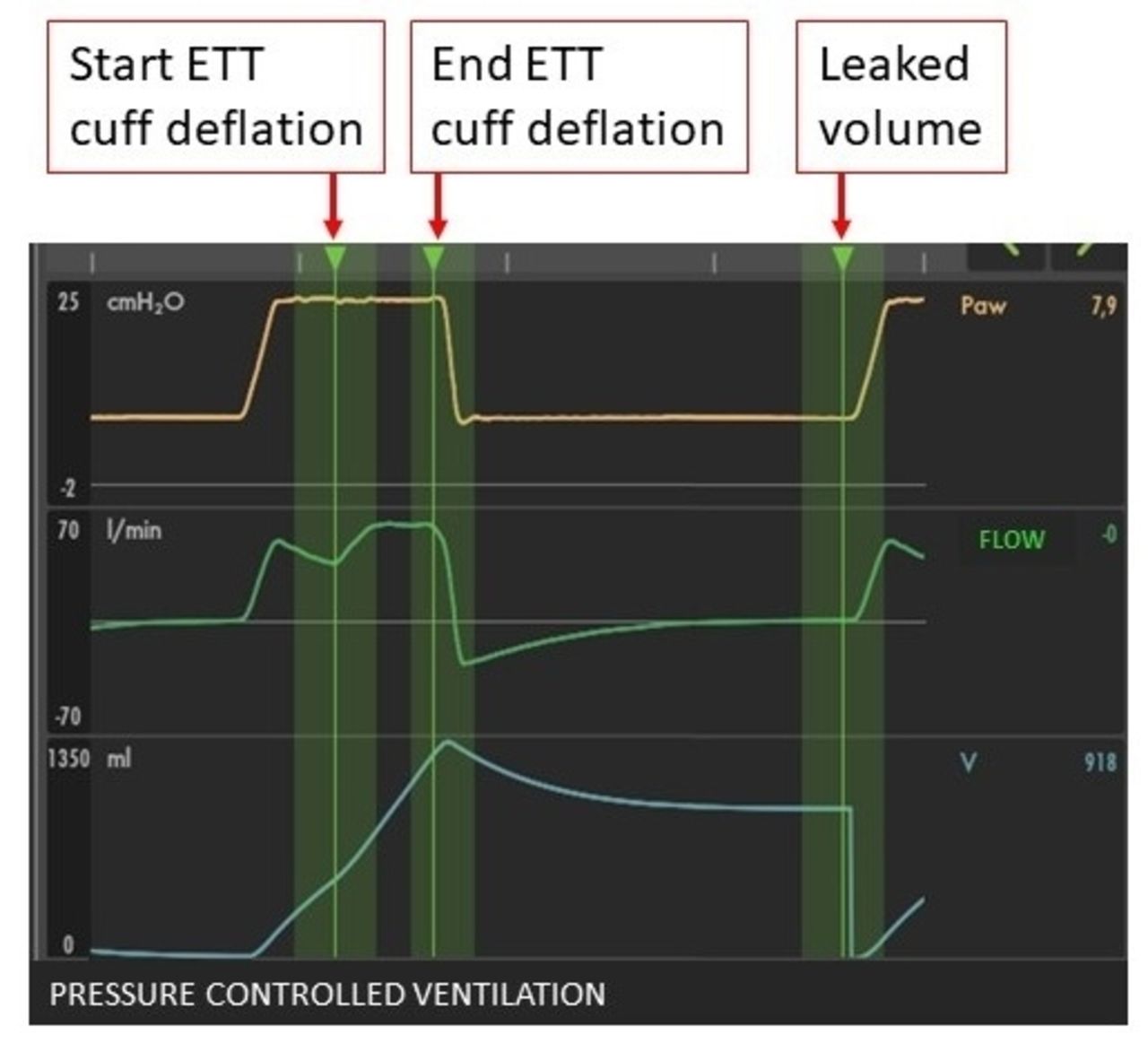
Patients undergoing invasive mechanical ventilation accumulate secretions into the trachea, both below and above the endotracheal tube (ETT) cuff. Therefore, suctioning is required to prevent complications due to secretion retention, but such a procedure is not without risks. TrachFlush is a new cuff controller synchronized with the mechanical ventilator that generates an artificial cough maneuver by briefly deflating and re-inflating the ETT cuff within the inspiratory time.
Methods:
7 patients admitted to our general intensive care unit were enrolled in the study and connected to TrachFlush (expected sample size 72 patients). A sigh (total inspiratory pressure 35 cm H2O, inspiratory time about 2 seconds, once per minute) was introduced if not present. The ETT cuff pressure was set to 25 cm H2O. We performed 3 artificial cough maneuvers during 3 consecutive sighs. The primary aim of the present study was to estimate the artificial cough flow generated around the ETT cuff, computed as the leaked volume divided by the cuff deflation time (average 1.18 s), see Figure 1. In 4 patients mouth aspiration was performed at the start and end of the study while in 5 patients endotracheal suctioning was performed at the end of the study. The study was approved by local IRB. Data are reported as mean ± standard deviation.
Results:
Table 1 reports the baseline data and the main results. All patients underwent 3 artificial cough maneuvers. All the artificial cough maneuvers in all patients produced an artificial cough flow ranging from 6.2 to 37.4 L/min. The mean flow was 21 ± 9 L/min. The average of the maximum flow reached in each patient was 28 ± 7 L/min. The maximum flow was recorded predominantly during the third cough maneuver. At the end of the study, in all the 4 patients in which mouth secretions were evaluated, we could detect secretions while endotracheal secretions were present in 4/5 of the patients. In one patient undergoing pressure support ventilation, the artificial cough maneuver stimulated the patient’s cough. No complications were recorded during the study.
Conclusions:
The tested ETT cuff controller was able to produce a significant artificial cough flow around the cuff promoting the transport of tracheal secretions, either sub-glottal or sub-cuff, into the mouth.
ETT#: endotracheal tube diameter, PEEP: positive end-expiratory pressure; Mouth and bronchial secretion were measured as 0 no secretions, 1 few secretions, 2 abundant secretions, 3 very abundant secretions; NE: not evaluated.
View all access options for this article.Table 1
Baseline
Artificial cough maneuver
Final evaluation
Patient
ETT#
Sex
Age (y)
Respiratory rate (bpm)
PEEP
Ventilatory mode
Tidal volume (ml)
Peak pressure (cmH2O)
Artificial cough flow (l/min)
MAX artificial cough flow (l/min)
Mouth secretions (0,1,2,3)
Endotracheal secretions (0,1,2,3)
1
7.5
male
19
15
5
Controlled
520
13
16.4±2.8
19.3
NE
NE
2
8
male
63
17
8
Assisted
450
13
10.4±6.4
17.8
1
3
3
7.5
male
63
19
6
Assisted
538
14
24.4±9.3
31
NE
NE
4
7.5
male
46
18
11
Controlled
331
26
28.5±6.7
33.6
NE
2
5
7.5
male
40
12
5
Controlled
653
23
19.8±6.5
25.4
1
0
6
7.5
female
79
15
7
Controlled
408
16
26.4±3.6
29
2
2
7
7.5
male
73
26
10
Assisted
504
23
18.7±16.2
37.4
1
1
TOT
55±21
17±4
7±2
486±103
19±6
20.5±9.2
27.6±7.2
Get full access to this article