
Abstract
Background:
The current and projected respiratory therapist staffing crisis requires a re-examination of the workload. In May of 2021, 9,086 nebulized treatments were delivered throughout our 700-bed academic medical center. Of those 9,086 treatments, 4,648 were non-evidence-based therapies; specifically 3% hypertonic saline (HTS) and acetylcysteine (NAC). Time spent delivering 4,648 non-evidence-based therapies was calculated to equal 6.7 full time employees (FTE). The aim of this value-based care initiative is to reduce the number of non-evidence-based treatments in an effort to optimize respiratory therapy resources.
Methods:
The number of inpatient 3% HTS and NAC doses administered by location and ordering provider were obtained from electronic medical record. These data were shared with ordering providers and the medical executive committee (MEC) and accompanied by the AARC Clinical Practice Guideline: Effectiveness of Pharmacologic Airway Clearance Therapies in Hospitalized Patients. The MEC voted unanimously to establish a policy empowering respiratory therapists to discontinue orders for 3% HTS and NAC in patients without an AARC guideline indication for treatment. The primary outcome measure was respiratory therapist time in FTEs for HTS/NAC administration and number of administered HTS/NAC nebulizer treatments. The identified strategic goal is reduction of time spent in FTEs.
Results:
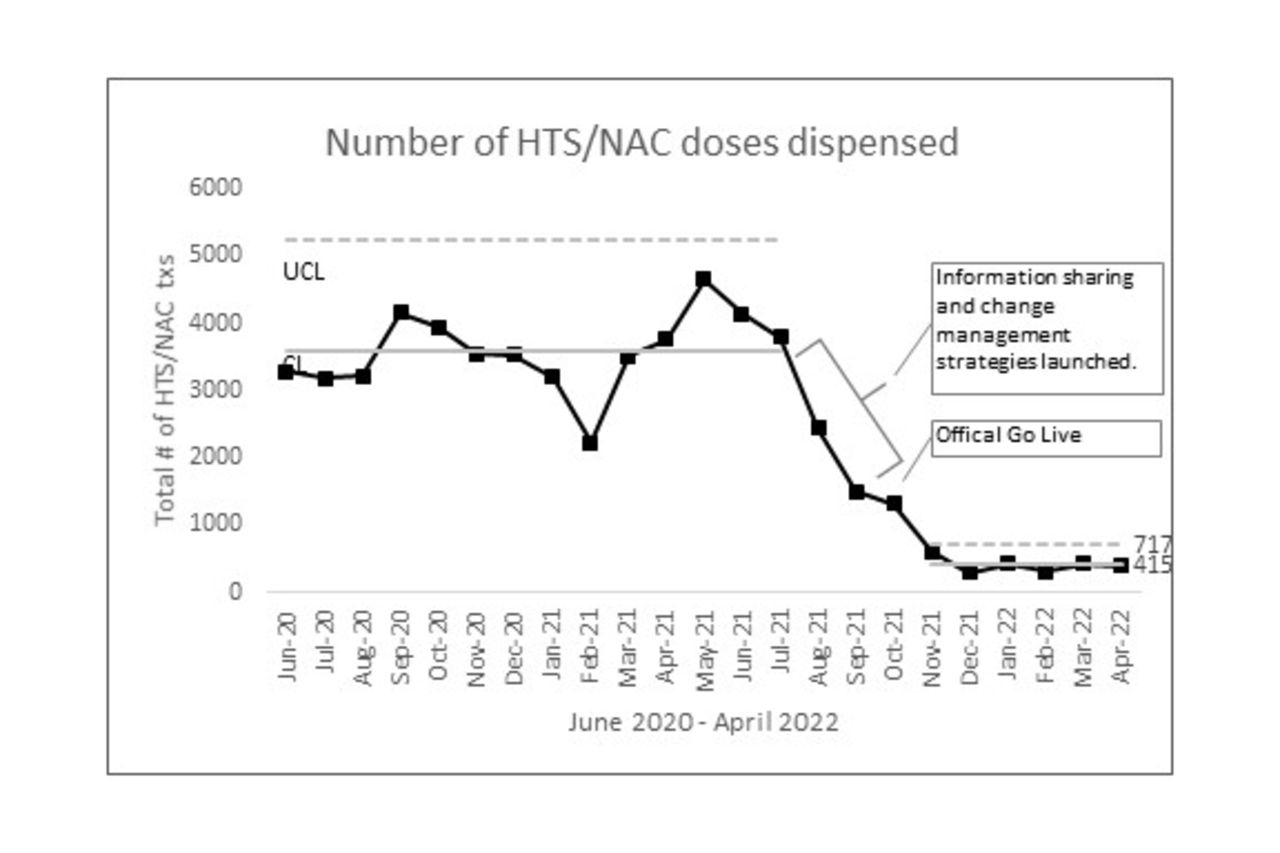
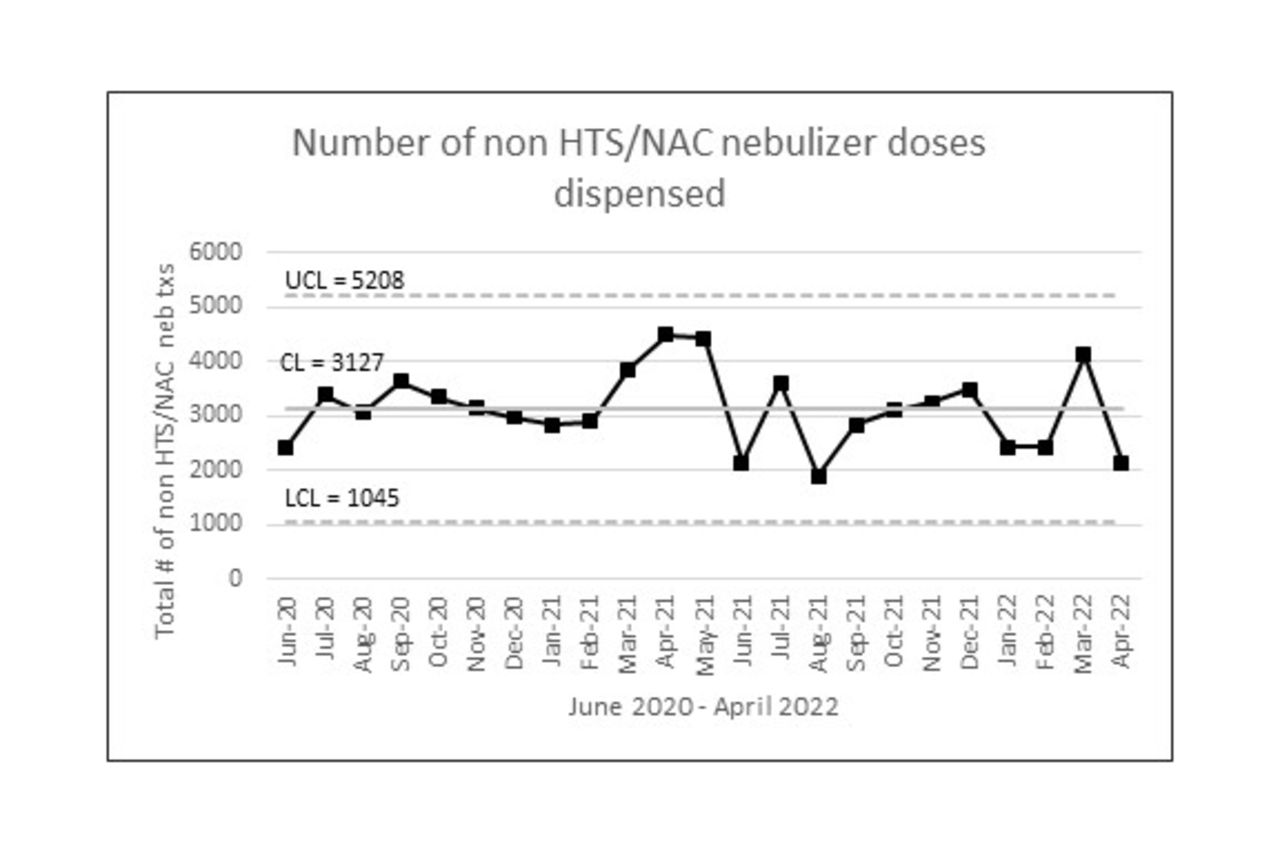
Change management strategies began in July 2021. The policy was implemented in October 2021. A control chart of HTS/NAC doses dispensed shows a marked decrease in median doses delivered from 3,582 pre-implementation to 415 post-implementation, while number of non HTS/NAC doses remained within control limits. Pre-implementation, median time in FTEs was equal to 5.2 versus post-implementation of 0.6 FTEs. Data were analyzed to account for daily census and days in month which was found to be 0.996 correlated with number of doses dispensed.
Conclusions:
Change management strategies supported by data, evidence, and policy can significantly reduce non-evidence-based therapies and optimize respiratory therapy resources in an academic medical center.
Get full access to this article
View all access options for this article.