
Abstract
Background:
Intrapulmonary percussive ventilation (Percussionaire, IPV) simultaneously delivers both aerosol and airway clearance. IPV can be administered in-line during mechanical ventilation with an adapter that remains in the ventilator circuit, decreasing the need for disconnection. The adapter has a pressure relief port that is adjusted during therapy when volume ventilation is used. Aerosol nebulization is known to generate fugitive aerosols, however the effect of opening the relief valve of IPV on fugitive aerosols is unknown.
Methods:
The aim of the study was to evaluate fugitive aerosols produced during IPV when administered in-line during invasive mechanical ventilation in a pediatric lung model. A ventilator (Maquet, Servo-i) was connected in series to a dual limb circuit, 5.5 pediatric endotracheal tube with cuff inflated, filter (to prevent aerosol from entering test lung), and test lung set to ARDS (resistance Rp20, compliance 10 mL/mbar). The adapter was placed in the inspiratory limb of the circuit at the y-piece. Ventilator settings were RR 20, VT 100, PEEP 10, I-time 1 in pressure regulated volume control mode. Variables were IPV pressure (25 or 40 psi), percussion (easy or hard), and adapter opening (closed, 25% or 50% open). IPV was operated for 15 min with 10 mL normal saline. A particle counter was placed 0.3 meters (1 foot) from the adapter opening. Three different IPV systems were used in each condition. Outcomes chosen to evaluate exposure were adjusted peak count (peak count – baseline count), time to baseline count after therapy, and percent of particles < 5µm (respirable range). Descriptive statistics were used to summarize results. Man-Whitney test was used to compare easy and hard settings. Kruskal-Wallis was used to compare different openings. A P value < .05 was considered statistically significant.
Results:
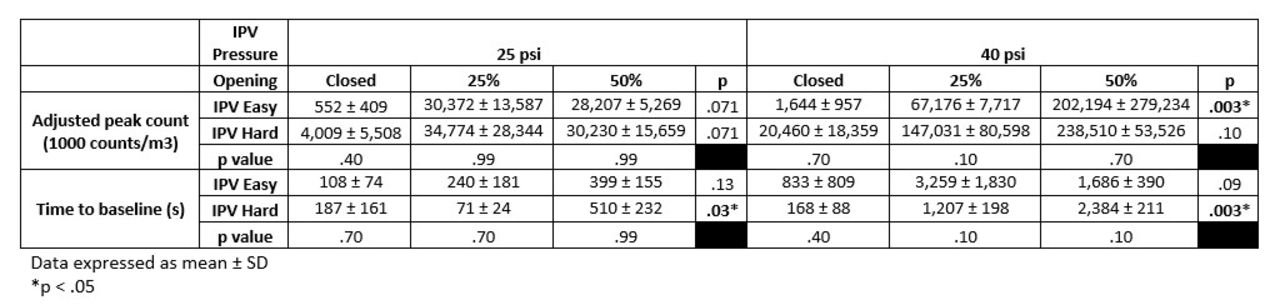
Percentage of particles < 5µm remained 99% or greater for all conditions. The use of an open adapter and 40 psi resulted in emission of larger amounts of fugitive aerosols. The use of hard IPV percussion resulted in longer times to return to baseline. Results were expressed as mean and SD.
Conclusions:
Almost all fugitive aerosols had a particle size in the respirable range. A large variation in outcome measures among IPV units was observed. Practitioners need to be aware of risk for prolonged aerosol exposure resulting from the use of in-line IPV with adjustable adapter.
Get full access to this article
View all access options for this article.