
Abstract
Background:
When mechanically ventilating the neonatal population, care must be taken because small changes in airway pressure or delivered volume can lead to adverse outcomes. Our aim is to determine the effect of tube compensation (TC) on the neonatal population. This could identify the advantages or disadvantages for its use and lead to better methods of ventilating neonates. We hypothesize that there will be no difference in tidal volume delivered, plateau pressure recorded, and static compliance measured when TC is active versus when it is inactive.
Methods:
Three different sized Shiley (Covidien, Mansfield, MA) cuffed ETTs (2.5, 3.0, 3.5mm) were used on two different ventilator platforms: Drager V500 (Lubeck, Germany) and Hamilton C6 (Bonaduz, Switzerland) with 100% TC, using the mode synchronized mandatory minute ventilation: pressure control with pressure support (SIMV (PC) + PS). For the test lung we used the Adult/Infant Training Test Lung model 5601i from Michigan Instruments (Grand Rapids, MI). Peak inspiratory pressure (PIP), plateau pressure (Ppl), dynamic compliance (Cdyn) and static compliance (Cstat) and tidal volumes (VT) delivered to the patient were compared using each ETT on both ventilators. Settings for each ventilator included a respiratory rate of 40, pressure control of 12 cm H2O, PEEP of 4 cm H2O, flow trigger of 0.5L/min, and an inspiratory time of 0.35 seconds. For each sized ETT on both ventilators, data was recorded with TC on and TC off. Statistical analysis was performed using R software (version 4.20).
Results:
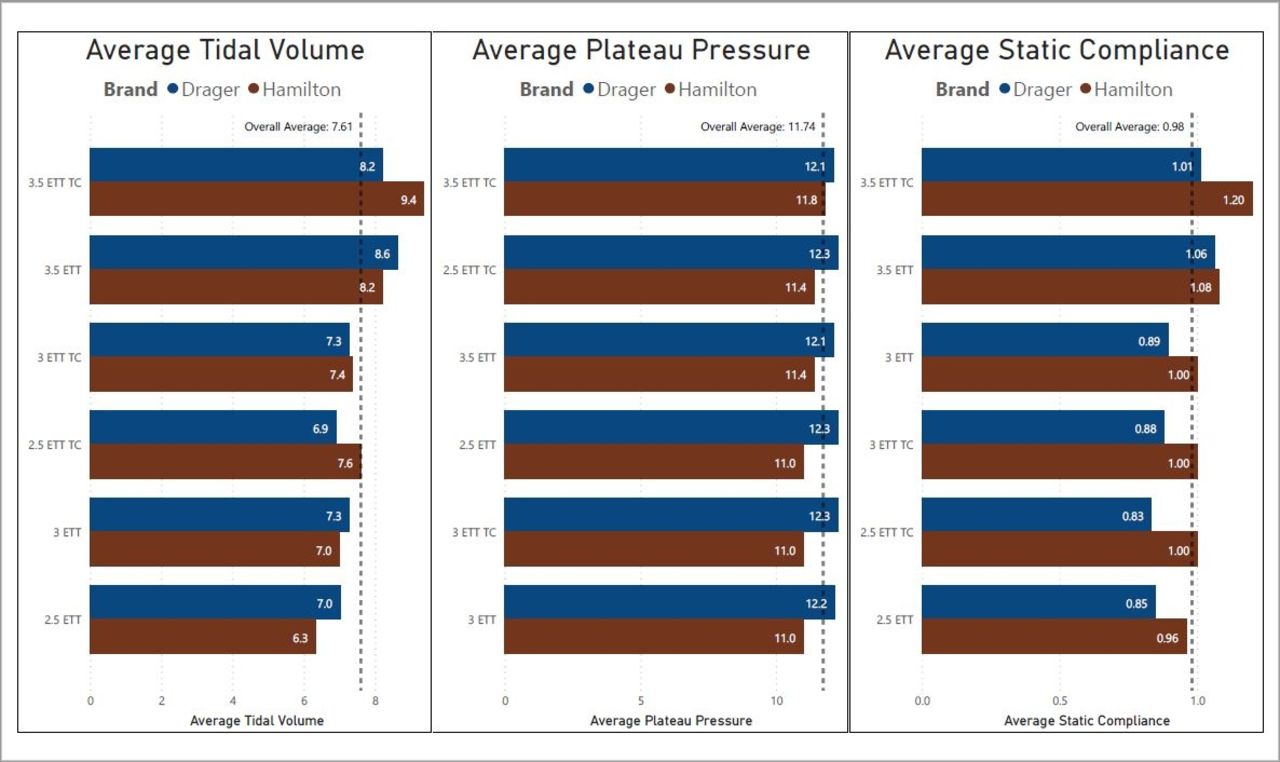
There was a significant increase in tidal volume delivered while TC was active (P = .02) and there was a difference in volume delivered based on ETT size (P <.001) and the interaction between ventilator brand and whether TC was active (P <.001). This was largely due to the Hamilton delivering larger tidal volumes on average. Ppl pressures were higher overall on the Drager (P < .001) but there was no difference in Ppl when TC was active (P = .07). Finally, static compliance was higher overall on the Hamilton (P < .001) and at larger ETT sizes (P < .001), but no different when TC was activated (P = .49).
Conclusions:
While the VT delivered when TC was active was increased, Ppl and Cstat were unchanged. It is unclear whether this could lead to volutrauma and adverse outcomes in the neonatal population. We reject the null hypothesis due to the difference in VT. More studies need to be done to determine if these results bear any clinical significance.
Get full access to this article
View all access options for this article.