
Abstract
Background:
In neonatal medicine, a ventilator’s inability to recognize and deliver patient triggered breaths can have serious consequences. Our goal is to analyze the effect flow sensor location has on spontaneous neonatal breaths in order to gauge any change in sensor responsivity. We hypothesize there will be no change in sensor response regardless of location.
Methods:
The following three ventilator platforms were tested: Draeger Infinity V500 (Lubeck, Germany), Hamilton C-6 (Bonaduz, Switzerland), and the Getinge Servo-U (Gothenburg Sweden). Both the Hamilton and Drager ventilators utilize a proximal flow sensor placement, while the standard Servo-U utilizes a distal flow sensor placement. Each ventilator was set-up in spontaneous mode, with a pressure support of 8 cm H2O, 4 cm H2O PEEP and a flow trigger of 0.3 L/min. The ventilators were connected to an Ingmar ASL 5000 test lung and breathing simulator (Ingmar Medical, Pittsburgh, PA). The ASL 5000 was set using the healthy neonate preset, with a compliance of 8 mL/cm H2O, Raw of 40 cm H2O/L/s and frequency of 40 breaths/min. Inspiratory muscle pressures (IMP) were set in a decremental fashion, at 5, 2.5, 1.25, and 0.75 cm H2O and the total number of breaths triggered in 1 minute was recorded at each IMP setting. Each pressure run, on all three ventilators, was performed in triplicate. Statistical analysis was performed using R (version 4.20) software.
Results:
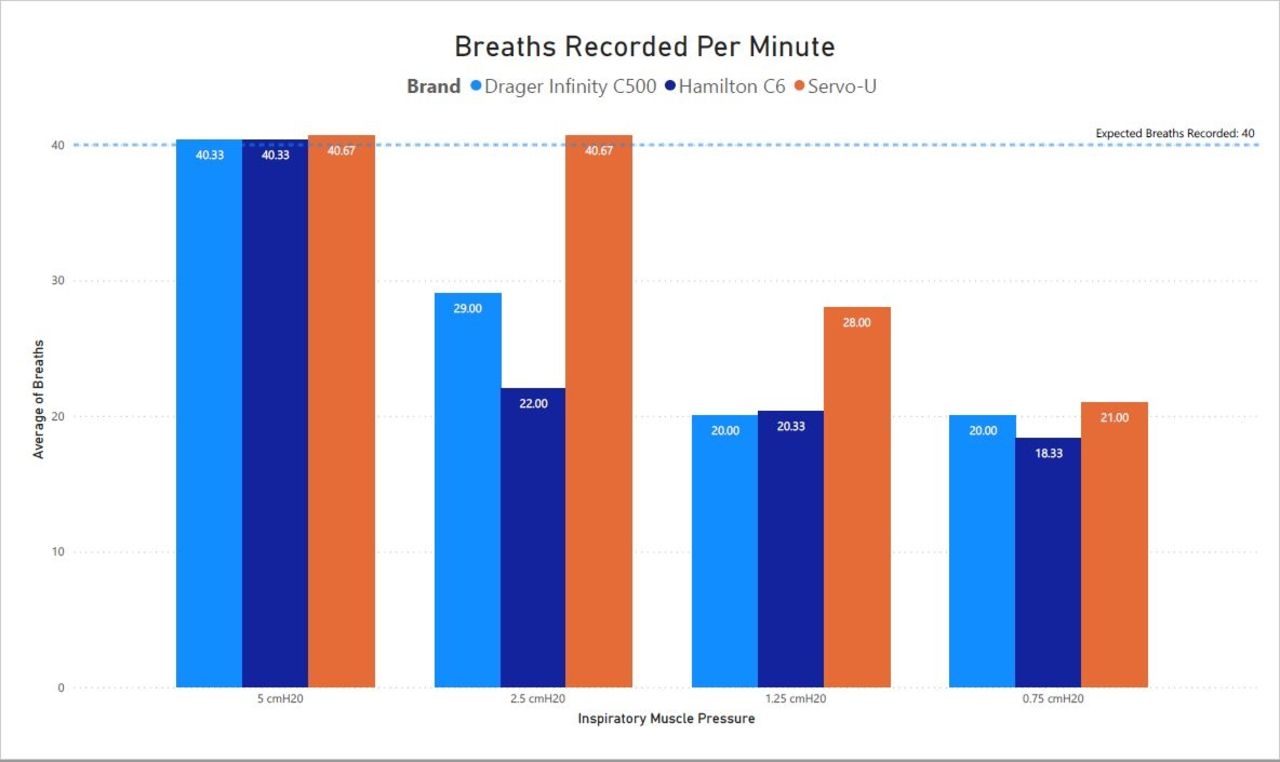
During the 5 cm H2O IMP trial, all 3 ventilators delivered 100% of the ASL set breaths. During the trial with a set IMP of 2.5 cm H2O the Servo-U continued to deliver 100% of the ASL set breaths followed by the Drager that delivered 55% of set breaths, while the Hamilton delivered 53% of set breaths. For the trial with a set IMP of 1.25 cm H2O the Servo delivered 70% of ASL set breaths compared to the Drager and Hamilton that delivered 50% of set breaths. The final trial with the IMP set at 0.75 cm H2O the Servo delivered 52% of ASL set breaths, the Drager delivered 50% of set breaths and the Hamilton delivered 45% of set breaths. There were statistically significant differences in the number of triggered breaths between brand of ventilator (P < .001), IMP set (P < .001), and the interaction between ventilator brand and IMP set (P < .001).
Conclusions:
While more testing should be completed, we conclude that the distal flow sensor on the Servo-U ventilator is more receptive to patient effort than the proximal flow sensors on the Drager V500 and Hamilton C-6.
Get full access to this article
View all access options for this article.