
Abstract
Background:
The COVID pandemic not only stressed the healthcare system, it also compromised all forms of medical education. Our department provides the bulk of our care in the ICU. All respiratory therapists (RTs) need to be proficient critical care providers. Our department recruits newly graduated RTs. As pandemic restrictions provided far less clinical instruction, we noticed new graduates were less prepared and less clinically exposed. We realized our prior orientation would be woefully inadequate to address this – therefore, we chose to enhance simulation-based learning (SBL).
Methods:
Our hospital has a fully equipped simulation center. With ten RTs who have been trained as simulation educators, we chose to enhance SBL. We segregated sessions into 3 categories: equipment, procedures, and clinical management. The equipment session entailed one-on-one training before the orientee managed the equipment in the hospital. The procedure session entailed one-on-one training to specific procedures (eg, mini-BALS.) Clinical management scenarios replicated high risk – low volume events that required advanced critical thinking (eg, airway emergencies). Each session was conducted by RT simulation instructors. The continuity of instructors and consistency of educational objectives was greatly enhanced. SBL time expanded from 8 hours to 40 hours.
Results:
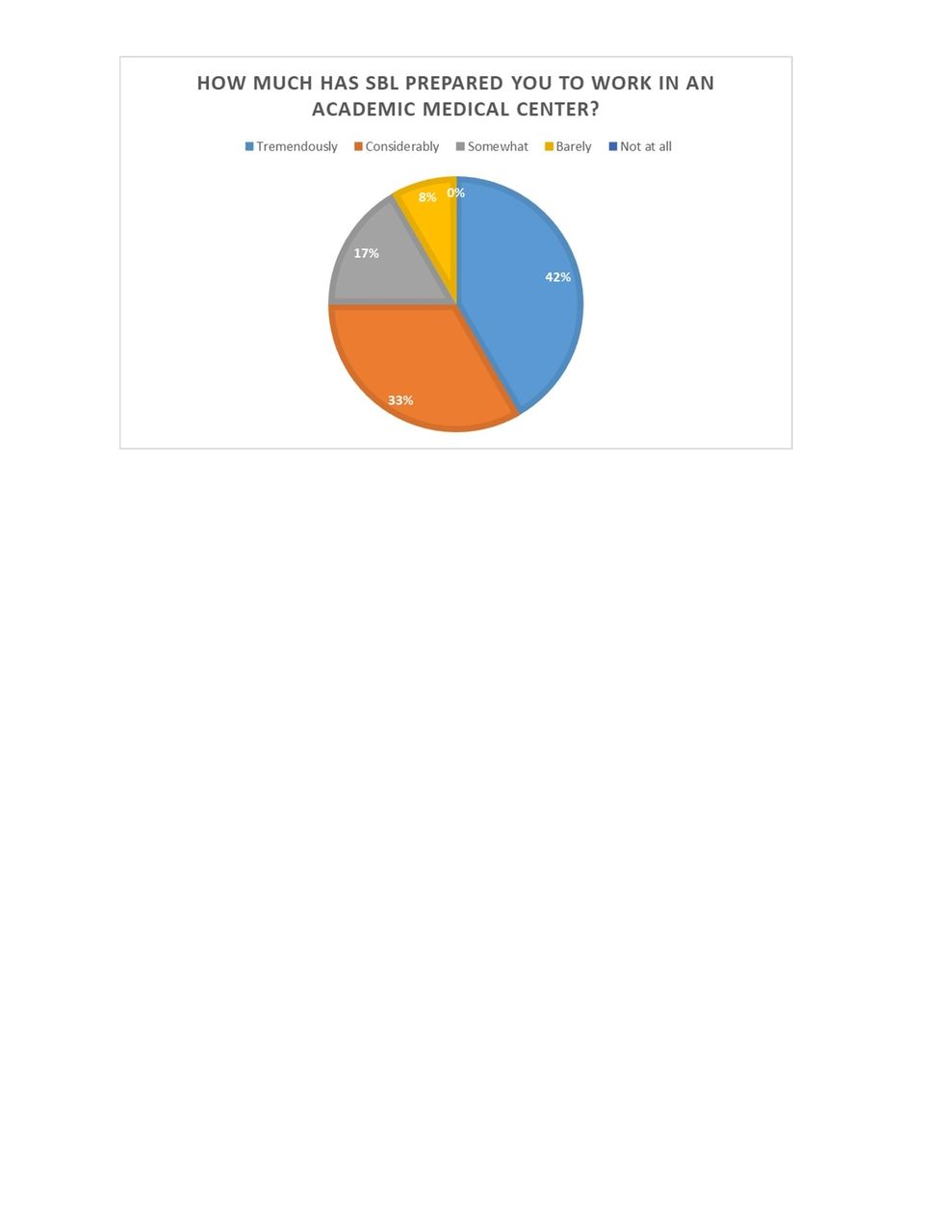
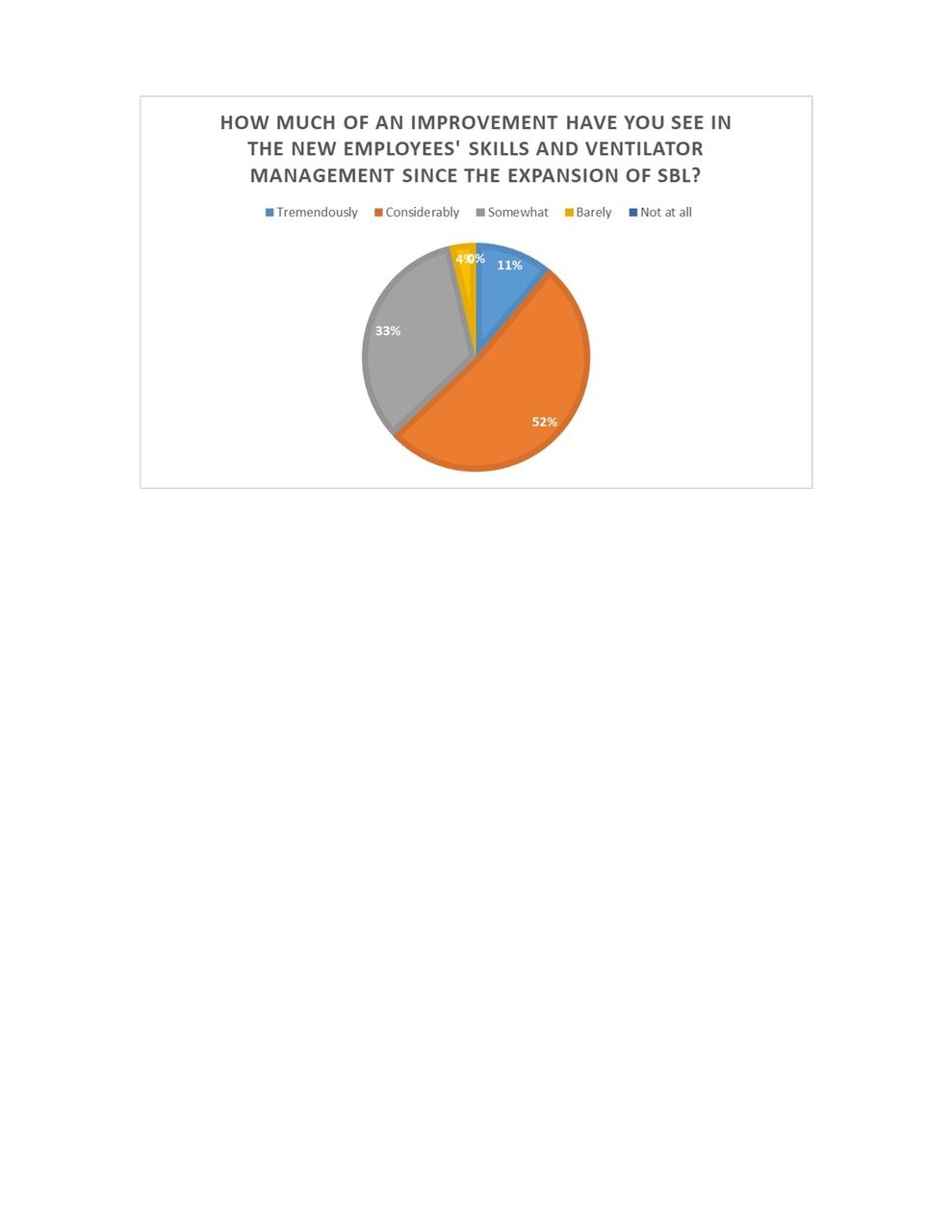
We surveyed existing RTs and new orientees as to the effectiveness of expanded SBL. All indicators showed improvement. Whenever we surveyed new orientees with expanded SBL, 75% felt SBL prepared them considerably. When asked if the amount of SBL should be changed, 46% felt SBL should be increased. No one felt SBL time should be decreased. Whenever we surveyed RT staff employed prior to enhanced SBL, 63% felt new employees’ skills and ventilator management improved considerably over employees without enhanced SBL. Whenever asked if they had seen an improvement in the way new employees managed emergencies, 56% saw significant improvement.
Conclusions:
Based upon results, an overwhelming majority felt expanded SBL proved beneficial. SBL consisted of highly trained instructors in a controlled and safe learning environment and repetitive practice. This proved far superior to random preceptors who rely upon chance opportunities to gain clinical practice for the orientee. Our traditional method of orientation exceeded $20,000 over a span of 14 weeks. Our future intention is to calculate the cost benefit of enhanced SBL orientation to traditional orientation.
Get full access to this article
View all access options for this article.