
Abstract
Background:
Mechanical ventilation (MV) is a life-saving intervention in critically ill patients. MV has side effects such as ventilator-induced diaphragm dysfunction (VIDD), with 80% prevalence in critically ill patients.1 VIDD results in longer ICU and hospital length of stay.2 Diaphragmatic training by repetitive noninvasive bilateral electromagnetic phrenic nerve stimulation could prevent or ameliorate VIDD.3 We have demonstrated that magnetic stimulation technology can be safely used in an ICU setting.4 We hypothesized that noninvasive stimulation of the phrenic nerves is feasible in anesthetized obese patients and results in a diaphragm contraction generating adequate tidal volume. The primary endpoint was the mean tidal volumes of at least 10 stimulations with the same intensity.
Methods:
This single center, proof-of-concept study was performed in five ASA I/II obese patients scheduled for elective surgery with general anesthesia and planned intubation after IRB approval and informed consent of each patient. After RSI induction anesthesia and intubation, patients received noninvasive electromagnetic stimulation of the phrenic nerves, while the mechanical ventilator was set on spontaneous breathing mode. For the stimulation, the STIMIT-exclusive PMR35 dual coils in combination with a standard clinical magnetic stimulator were used bilaterally with different stimulation intensities (30%, 40%, 50%).
Results:
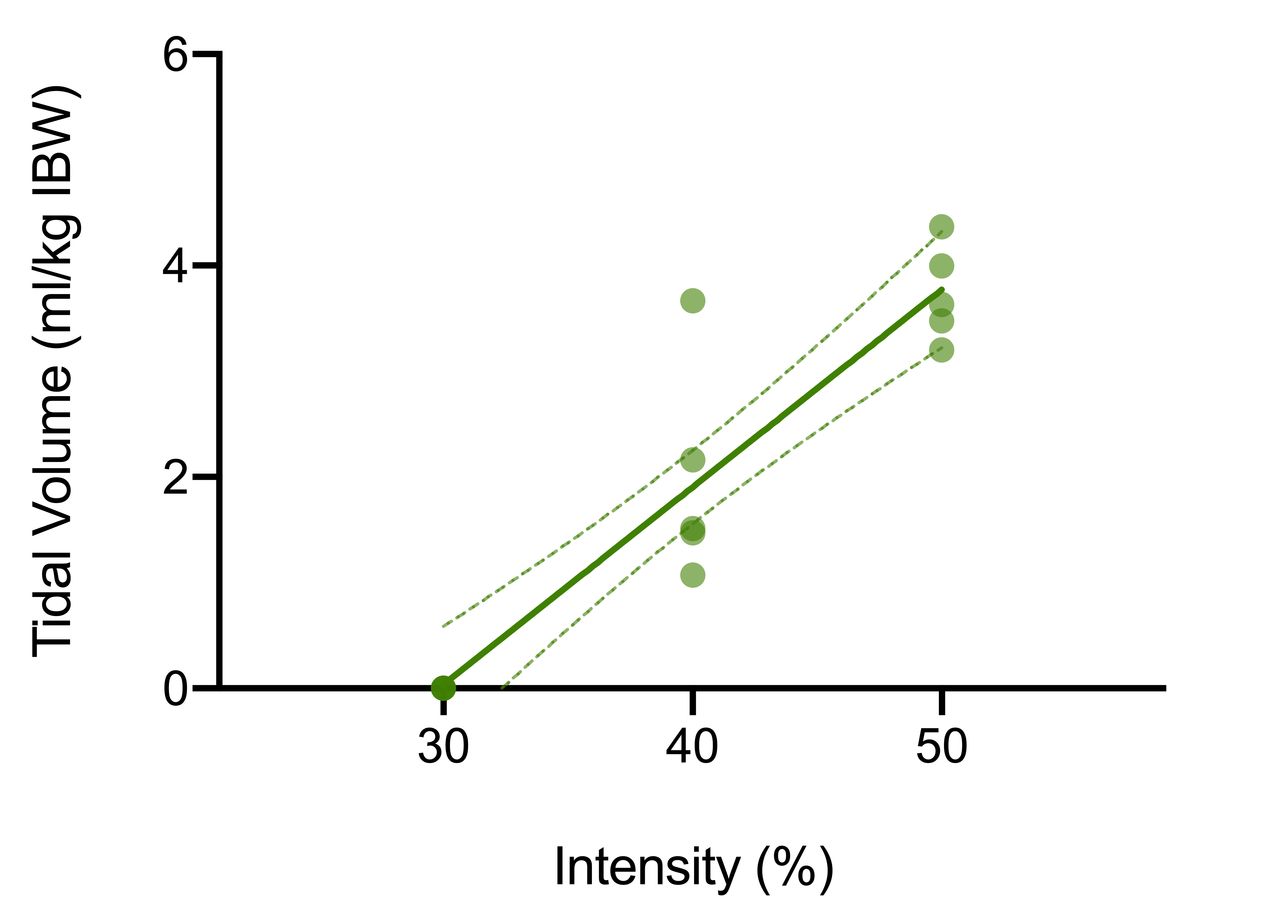
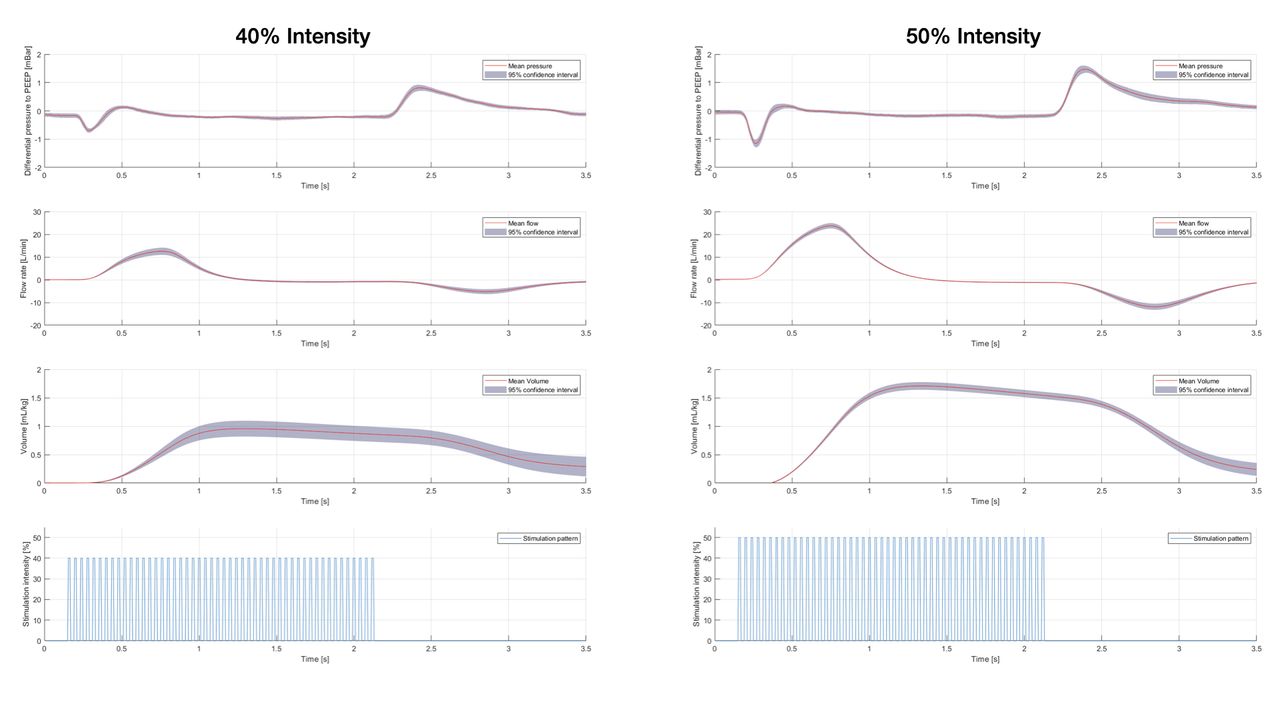
Patients were 34 [IQR 24-41] years old, 80% (n = 4) females, with a BMI of 42.7 [IQR 38.0-46.6] undergoing elective surgery. The mean tidal volume was 0.00 ± 0.00 mL/kg ideal body weight (IBW), 1.97 ± 1.02 mL/kg IBW and 3.73 ± 0.45 mL/kg IBW for 30%, 40% and 50% stimulation intensity, respectively (Figure 1). There was a linear relationship between dosage (stimulation intensity) and effect (tidal volume) (P < .001; r2 = 0.87). The stimulation intensity to induce 3-6 mL/kg IBW was 50% intensity in most cases (Figure 2).
Conclusions:
Noninvasive bilateral phrenic nerve stimulation can effectively generate diaphragm contraction. A stimulation intensity of 50% generated diaphragm contraction induced tidal volumes of 3-6 mL/kg IBW in pulmonary healthy, obese anesthetized patients. Whether this non-invasive technique can prevent or attenuate VIDD should be assessed in critically ill patients. References: 1. Jung B, et al. ICM. 2016; 42: 853-861. 2. Goligher EC, et al. Am J Respir Crit Care Med 2018;197:204-213. 3. Reardon PM, et al. Curr Opin Crit Care 2021;27:282-289. 4. Kuhn KF, et al. SciRep 2021;11:16317.
Get full access to this article
View all access options for this article.