
Abstract
Background:
Past studies have supported the superiority of flow triggering during mechanical ventilation. Pneumotachometers that are placed proximally to the patient have shown to provide more accurate measurements for the changes in volume, airway pressure, and gas flow. Therefore, a ventilator system such as the Hamilton G5 with an external flow sensor that is proximal to the patient will be more sensitive in responding to a patient's efforts.
Methods:
The ASL 5000 high fidelity lung simulator (IngMar Medical) was used to simulate a breathing pattern on the Hamilton and Avea ventilator systems. Both ventilators were set with the same ventilator settings, which included a flow trigger setting of 2.5 L/min and a bias flow of 5 L/min. The same ventilator circuit and flow sensor (Hamilton G5) was used in all of the trials. The same lung characteristics on the ASL 5000 were used in all of the trials. The ASL 5000 was run for 10 breaths on three different Hamilton G5 and Avea ventilators. The average time-to-trigger was calculated for each of the six trials using the ASL software.
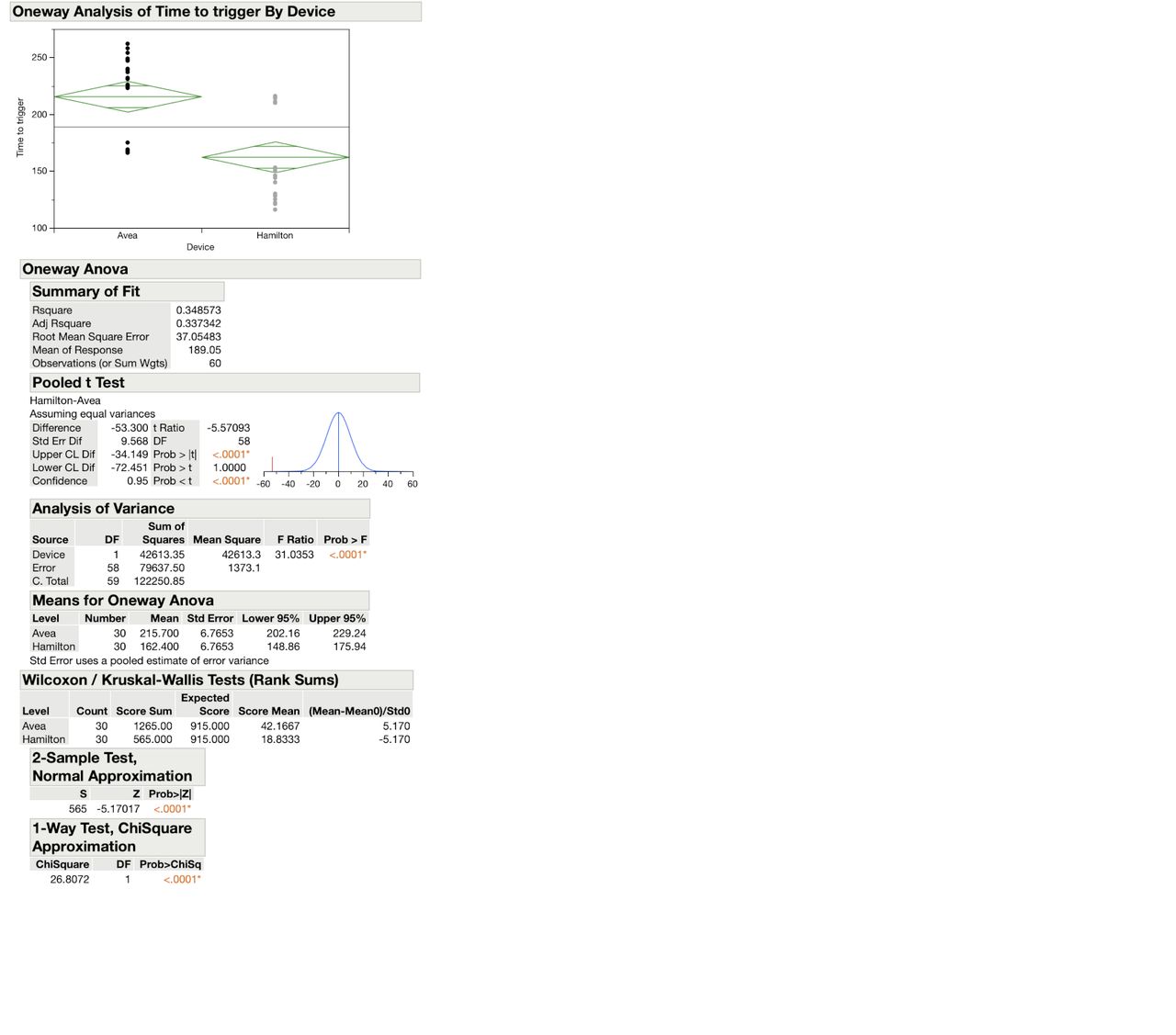
Results:
The average time-to-trigger in the Hamilton ventilators was 162.4 ms compared to 216 ms in the Avea ventilators. However, there was a wide, unexpected variance in samples within each device. Within the Avea ventilators the analysis of variance shows an F Ratio of 499.9 (P < .001). In the interval plot, AVEA ventilator #1 had the fastest time to trigger response, and the least amount of variance. The AVEA ventilators #2 and #3 had a slower time to trigger response but had a wide variance in values. The Hamilton G5 ventilators #1 and #3 were significantly quicker to respond to triggers than Hamilton ventilator #2, but there was a significant variance between the three devices. A 2-sample t-test shows that the data is significant.
Conclusions:
The test runs show that there is a significant variance between the time-to-trigger within both devices. However, 2 of the 3 Hamilton ventilators demonstrated a faster time-to-trigger response than the Avea ventilators with the same flow trigger setting and bias flow. Further research is needed to address the wide variation in values in both devices. For example, the Hamilton G5 ventilators that were used had over 1,000 hours of usage and had not been serviced or calibrated. Only one flow trigger and bias flow setting was used during testing. Adjusting the bias flow and flow trigger could have significant effects on how quickly the ventilator will respond to the ASL 5000.
Get full access to this article
View all access options for this article.