
Abstract
Background:
Instillation via artificial airway is used to directly deliver medications into the trachea. Despite poor evidence, various medications have been reported as administrable via artificial airway. Different procedures are reported for administering medications via artificial airway but the efficacy of these methods has not been widely studied.
Methods:
This bench study utilized 3.5 and 6.0 tracheostomy and endotracheal tubes. Four volumes of sterile water (0.1, 0.5, 1.0, and 3.0 mL) were instilled down each airway using three repetitions and methods of instillation in random order. Methods included direct administration of water down the airway via syringe, advancement of a closed suction catheter (8 and 12 French for 3.5 and 6.0 tubes respectively) into the hub followed by administration of water through the instillation port of the suction catheter, and advancement of a closed suction catheter just beyond the tip of the airway followed by administration of water through the instillation port of the suction catheter. After instillation the catheter was withdrawn when applicable and five positive pressure breaths delivered to simulate mechanically ventilated breaths. Administered volumes were weighed pre/post instillation on a laboratory scale. Descriptive statistics and one-way ANOVA were used to compare mean volume differences, or volume lost, within and between each instillation method.
Results:
Mean difference in volume lost was homogenous across four volumes and three instillation methods. There was no statistically significant difference between mean volume lost for each method using the 6.0 tracheostomy or endotracheal tube. However, the mean volume lost for the direct instillation method for the 3.5 tracheostomy (P = .04) and endotracheal (P = .03) tubes was statistically significant compared to the other instillation methods for these airway sizes (Table 1).
Conclusions:
Instillation of sterile water down an artificial airway yields small volume differences between amount instilled versus amount recovered. Though direct instillation for the 3.5 tracheostomy and endotracheal tubes was significantly different statistically, the volume difference was not clinically significant. This data suggests that it may be more valuable for the clinician to weigh other considerations such as PEEP requirement, risk of infection, or overall patient tolerance when deciding which method is optimal for medication delivery to the trachea.
Table 1. Summary of mean volume lost (mL) by method and airway size and type.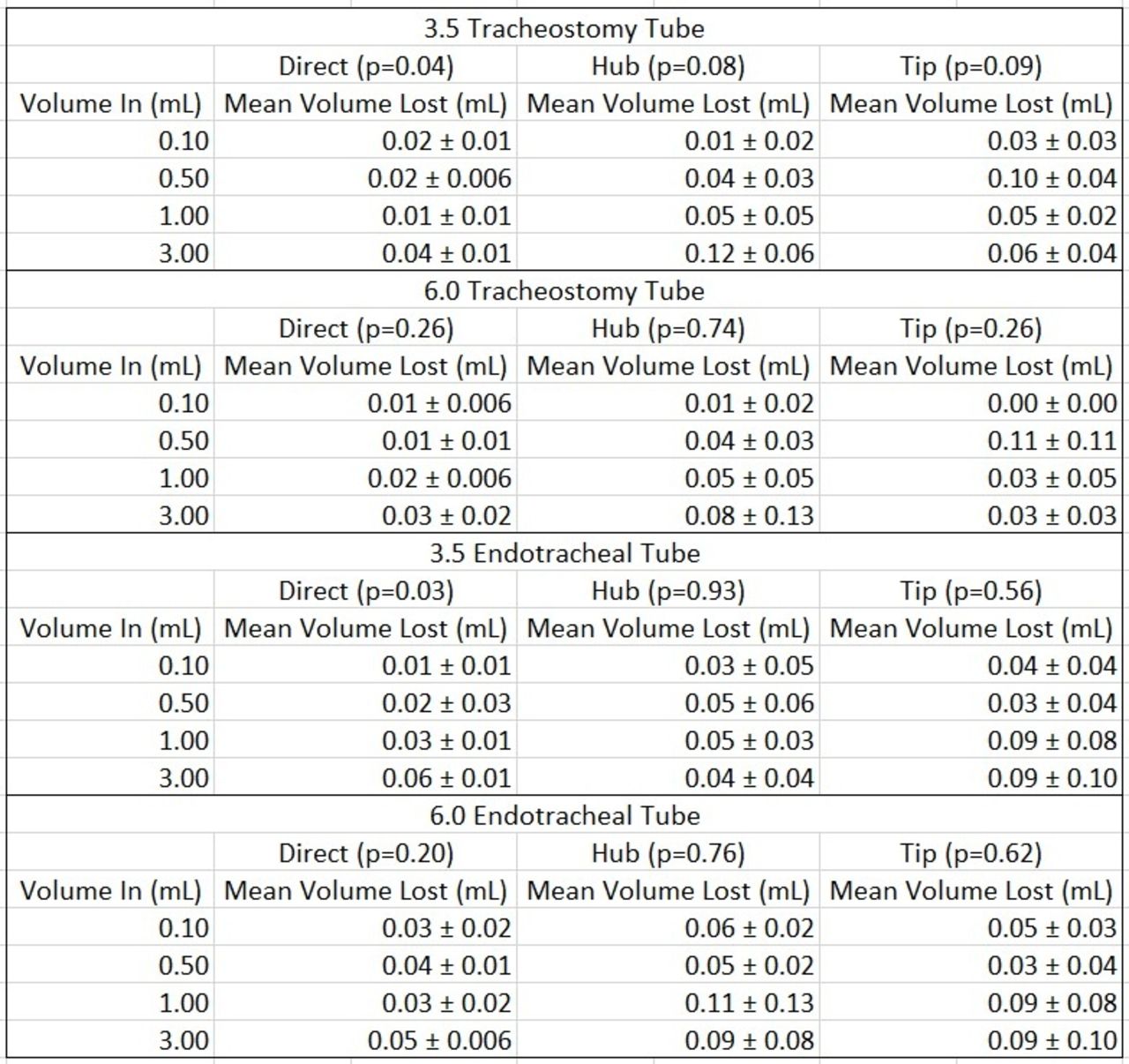
Get full access to this article
View all access options for this article.