
Abstract
Background:
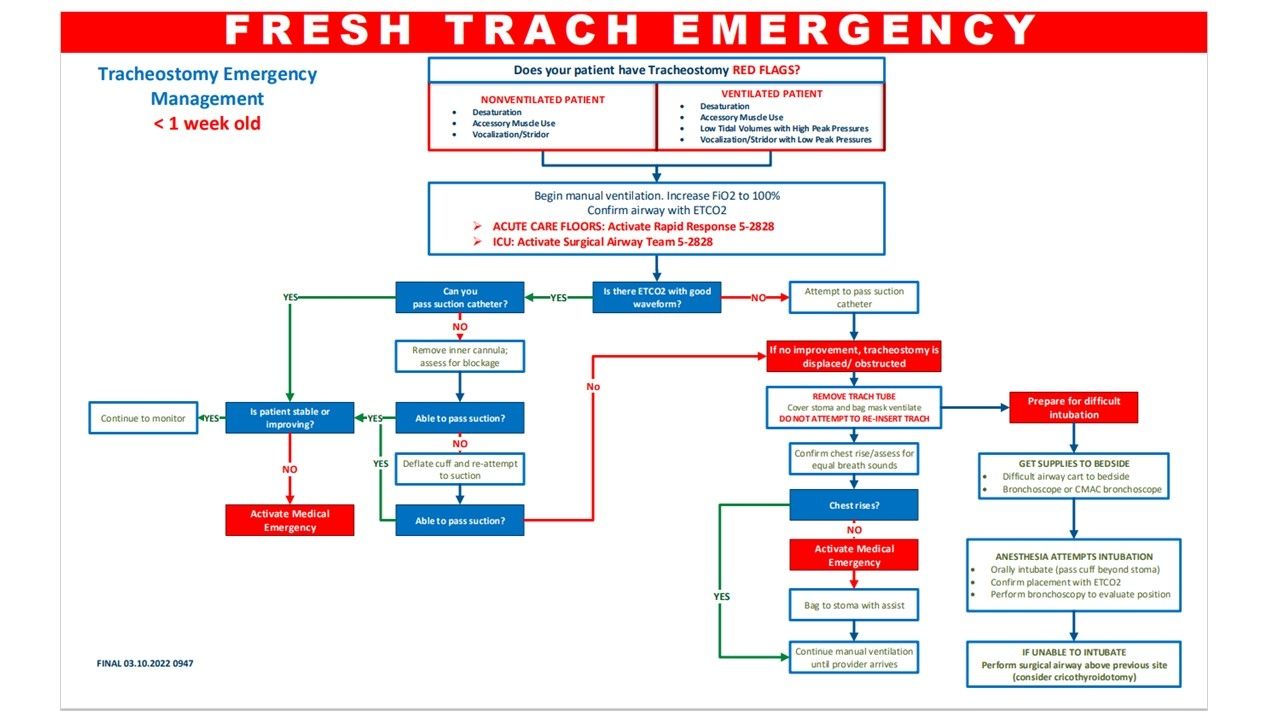
From July 2019 to January 2020, four sentinel events occurred related to accidental tracheostomy tube decannulation within our 700-bed academic medical center. Evaluation of these events by an inter-professional team comprised of RTs, intensivists, anesthesiologists, and patient safety specialists found that there was no consistent approach for early recognition and intervention of this type of surgical airway emergency at our facility.
Methods:
Following the inter-professional team review of the safety events, a literature review was conducted with focus on an evidence-based approach to prevent, identify, and provide timely interventions in patients with a suspected accidental tracheostomy decannulation. A tracheostomy surgical airway emergency workflow was developed and approved by the Safety Oversight Committee. Education consisting of computer-based learning and live presentations was provided to over 1,000 staff members including RTs, RNs, CNAs, and providers. RTs also participated in a high-fidelity simulation with focus on application of the emergency algorithm and team lead role demonstration. Implementation of the Surgical Airway Emergency Team (SAET) comprised of RTs, a rapid response RN, a medicine ICU resident, an ICU pharmacist, an ICU RN, an anesthesiologist, and a trauma surgeon was established to rapidly deploy trained clinicians for this type of emergency. Upon activation of the SAET, the RT will lead the stepwise algorithm interventions until the trauma surgeon assumes the role of team lead. The SAET went live January 1, 2021.
Results:
Since the introduction of the standardized approach for early recognition and emergency activation for suspected accidental tracheostomy decannulation in 2021, the SAET has been activated 10 times (1/1/2021-5/31/2022). No sentinel events have been associated with accidental tracheostomy tube decannulation since implementation. Data are collected and shared with the inter-professional Surgical Airway Practice Standardization workgroup, and Plan-Do-Study-Act (PDSA) cycles are used to identify and address opportunities for improvement in real time.
Conclusions:
A standardized approach empowers clinicians to have heightened safety awareness, identify early warning flags, and escalate care when appropriate that leads to improved patient outcomes. A quality improvement process with inter-professional clinicians maximizes resources and strengthens practice change. Ongoing PDSA cycles allow for continued progress for positive outcomes.
Get full access to this article
View all access options for this article.