
Abstract
Background:
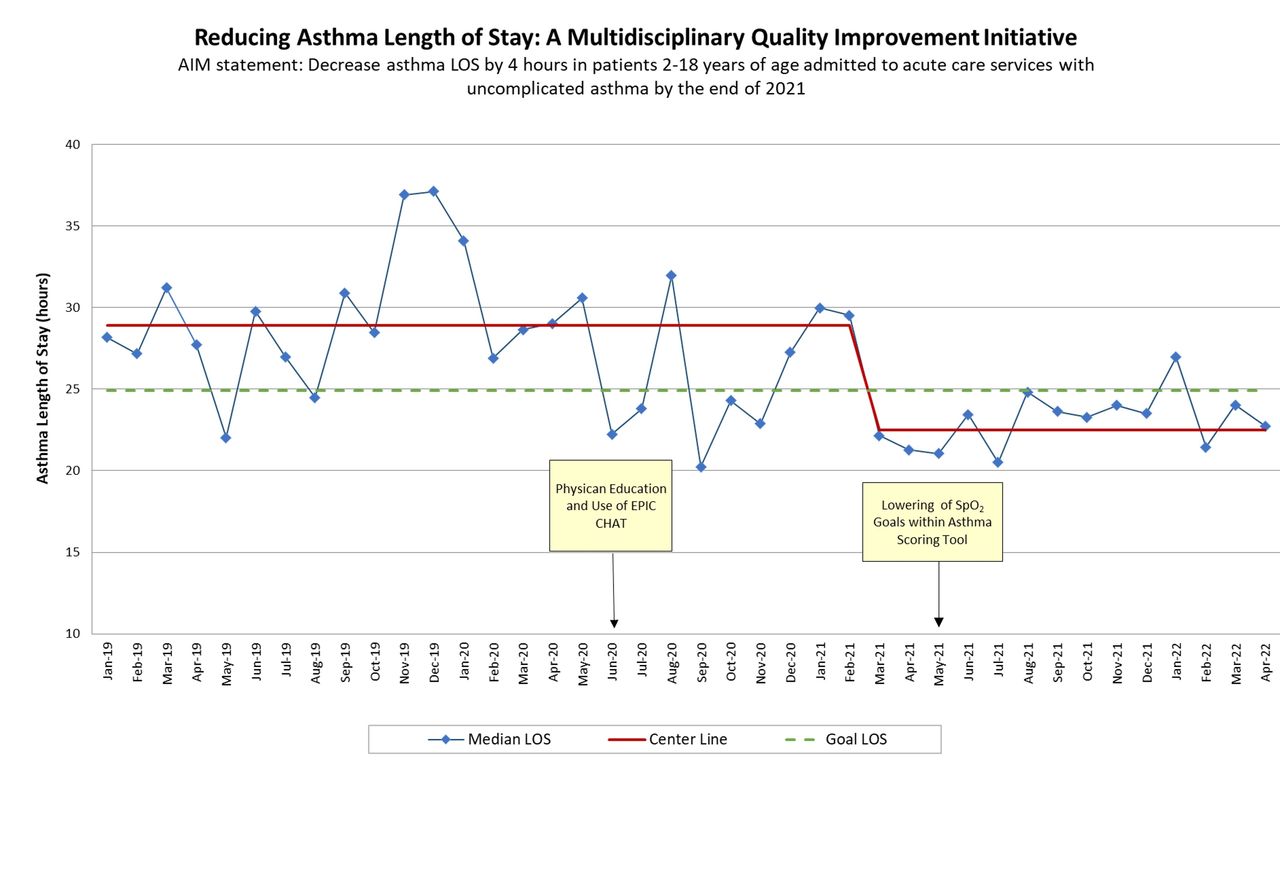
Acute asthma exacerbation is a leading cause of pediatric hospitalization and is associated with significant healthcare resource utilization and cost. Length of stay (LOS) is commonly used as a measure of efficiency, efficacy, and resource utilization, and even small reductions in LOS can substantially reduce the economic burden and impact on healthcare systems. To align with the top-10 Benchmark Hospitals among PHIS (pediatric health information system) for asthma LOS, we developed a multidisciplinary team consisting of pediatric hospital medicine providers and respiratory care leadership with the aim of decreasing asthma LOS by 4 hours in patients 2-18 years of age admitted to acute care services with uncomplicated asthma by the end of 2021.
Methods:
Utilizing the Model for Improvement, we identified three primary drivers possibly contributing to increased LOS: 1) A drift in the number of recommended (per our asthma clinical practice guidelines) treatments given before discharge, (2) the lack of an efficient and timely method for respiratory therapists to communicate with providers once patients had reached discharge criteria, and (3) stringent SpO2 goals within our asthma scoring tool. Adoption and implementation of interventions occurred in June 2020 and May 2021, which included: (1) provider education; (2) implementation of a chat feature within our EMR software system that allows respiratory therapists to send a message from the patient’s chart directly to the provider’s phone once a patient is ready to assess for discharge; and (3) lowering of SpO2 goals within our asthma scoring tool. Baseline median LOS for the 18 months prior to interventions was 28.9 hours. 30-day same-cause readmissions were used as balancing metrics. Rank sum and two proportion Z-test were used for statistical analysis.
Results:
For the 18 months (July 2020 to December 31, 2021) post first intervention, median LOS significantly decreased by 5.5 hours compared to baseline [23.4 hours (16.8-35.0) (n = 780) vs 28.9 hours (20.7-40.7) (n = 795), P < .001], with no difference in 30-day same-cause readmissions [pre 9.9% (79/795), post 8.3% (65/780), P = .308].
Conclusions:
Utilization of a multidisciplinary quality improvement initiative led to a significant decrease in asthma LOS without affecting 30-day readmissions. Next steps include protocolization of continuous short-acting beta-agonist (SABA) administration and evaluating frequency of SABA administration prior to discharge.
Get full access to this article
View all access options for this article.