
Abstract
Background:
Physician orders for life-sustaining treatment (POLST) forms are commonly signed by seriously ill patients and those with terminal cancer in order to improve their end-of-life care by specifying the extent and type of life-sustaining treatments (LSTs) that they wish to receive, thus enabling an appropriate preparation for their end-of-life months ahead of time. In contrast, patients with chronic lung diseases (CLDs) are often unable to sign the POLST form themselves because CLDs are characterized by recurrent episodes of exacerbation and recovery, which hinders an accurate estimation of their end of life. As such, POLST forms for CLD patients are often signed by their caretakers while the patients have become unresponsive in ICUs, which is not in line with the primary purpose of the POLST form. We therefore examined the characteristics and outcomes of CLD patients whose POLST forms were signed in the ICU.
Methods:
We retrospectively analyzed the medical records of 59 adult patients (male, 66%; mean age, 65.7 ± 12.2 years) with CLD whose POLST forms were signed at the ICU of our center between January 2019 and July 2021. Patients with cancer were excluded.
Results:
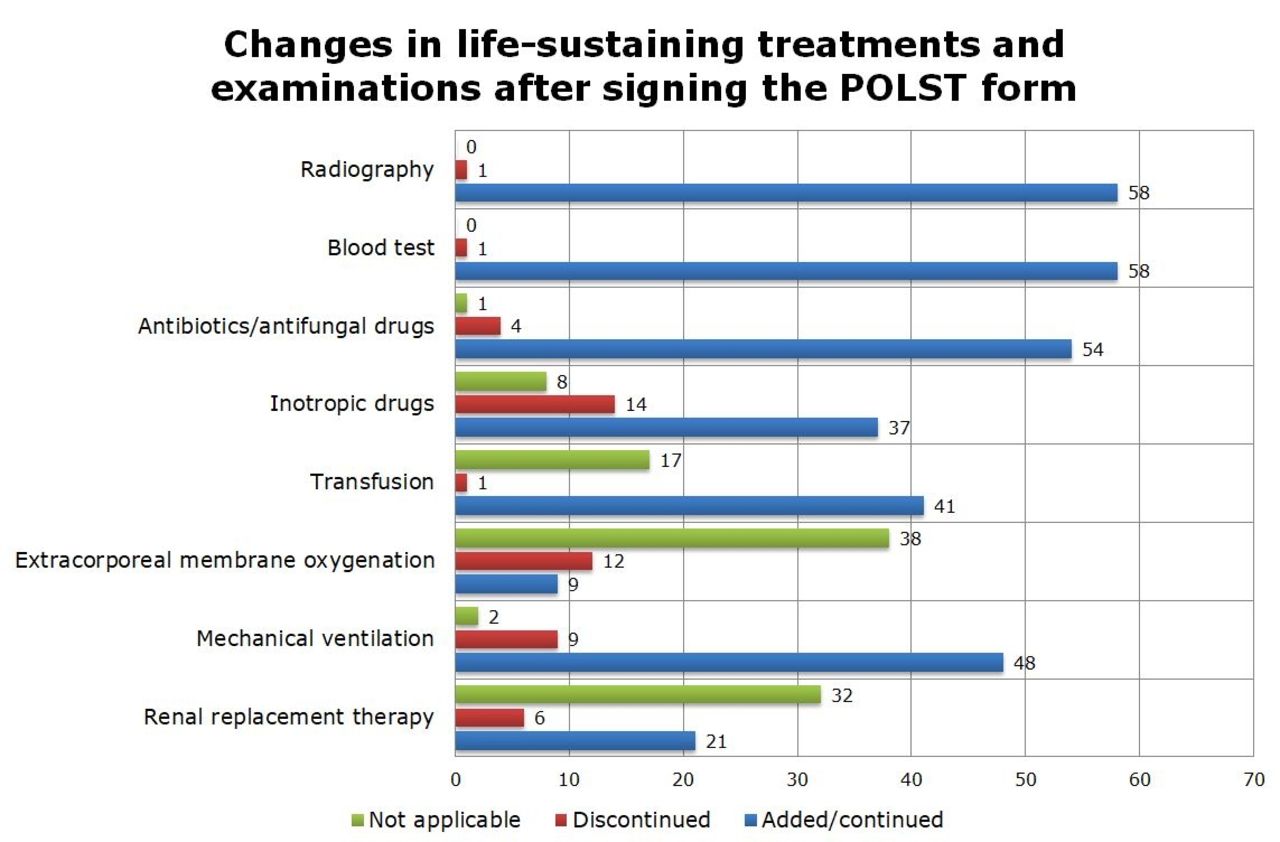
Of the 59 study patients, 58% had interstitial lung disease (ILD) and 27% had COPD. The main reasons for ICU admission were acute respiratory failure (58%), acute exacerbation (29%), and cardiac arrest (14%). At POLST decision, only 7% were fully alert and the POLST forms were signed by the caregivers in 97% of the cases. The rates of ICU mortality and in-hospital mortality were 90% and 93%, respectively; importantly, 58% died within 48 hours of the POLST decision. After the POLST decision, 98% of the patients still underwent blood tests and radiography. Antibiotics and mechanical ventilation were continued in 92% and 81% of patients. Inotropic drugs (24%), extracorporeal membrane oxygenation (20%), and mechanical ventilation (15%) were discontinued only in some patients after POLST.
Conclusions:
Virtually all POLST forms for CLD patients were signed by caregivers, and more than half were signed within 48 hours before death. Despite the POLST decision, intensive care methods were continued or added in many patients. These results suggest that in the case of CLD patients, it is necessary to discuss the patient's life-sustaining treatment plan in advance.
Get full access to this article
View all access options for this article.