
Abstract
Background:
Length of stay (LOS) is an indicator of efficiency of hospital management. Reducing LOS has been proven to decrease the risk of opportunistic infections, improve quality care, and lower mortality rates. An interdisciplinary team was implemented to initiate and evaluate strategic interventions that could facilitate discharge planning. Members included respiratory therapy (RT), nursing (RN), physicians, advanced practice providers, speech, physical, and occupational therapies, and case management. Goals included reducing LOS, coordinating care teams, and engaging clinicians by utilizing evidence-based protocols. Causes of increased LOS include weaning protocol not ordered or followed, inadequate RT documentation, and not progressing in therapies.
Methods:
Metrics and data were collected retrospectively through chart review pre- and post- interventions after IRB approval. Interventions include utilization of an evidenced-based RT-driven protocol, daily rounding between RN, RT, and provider, and a weekly interdisciplinary meeting to discuss barriers and synchronize care from multiple disciplines. 32 patients were identified in the pre-intervention group and 31 patients were in the post intervention group. Inclusion criteria included >18 years of age, tracheostomy present, mechanically ventilated, and weaning patient. Exclusion criteria included no-wean patient, home ventilator patient, and deceased during hospital admission.
Results:
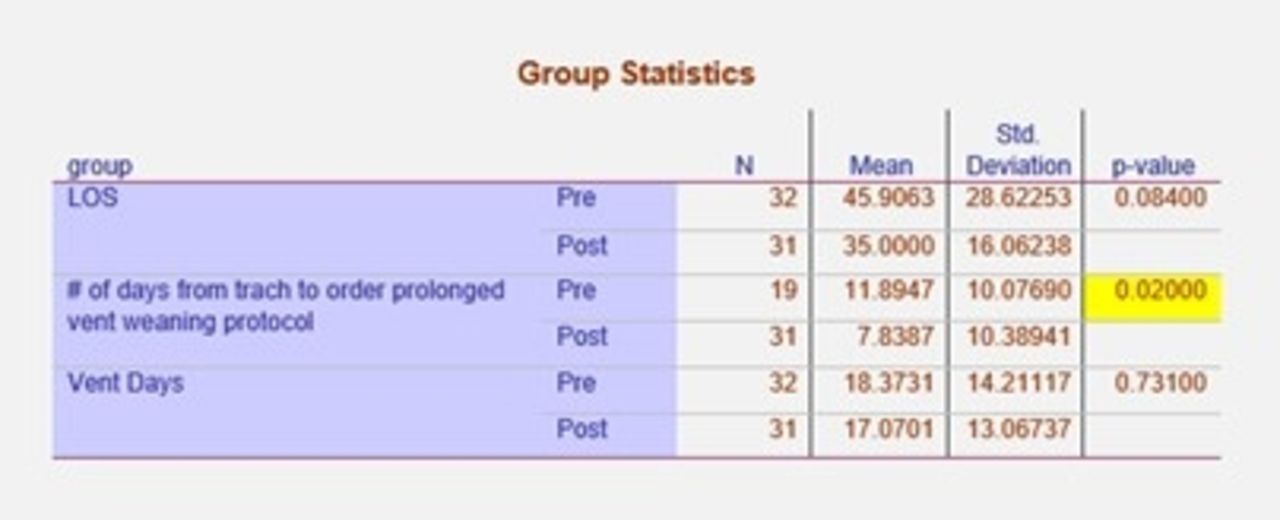
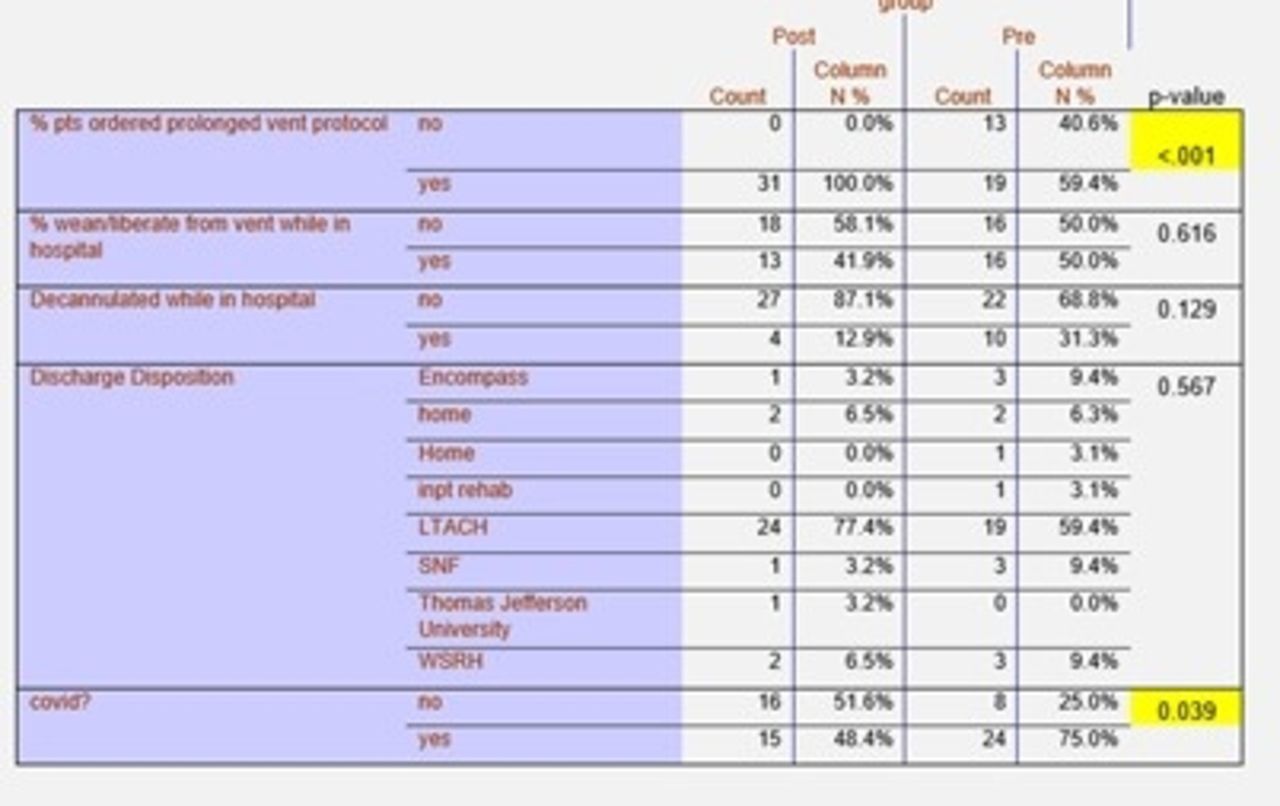
All data were analyzed through IBM SPSS software v25 (IBM, Armonk, New York) using chi-squared tests and independent samples t-test. Our study showed a clinically relevant reduction in mean LOS of 10.91 days (P = .084), this resulted in potential cost savings of approximately $216,455. In addition, there was also a 1.3-day reduction in ventilator days (P = .731), a significant reduction of 4 days from tracheostomy placement to protocol initiation (P <.02), and significantly more patients (40%, P <.001) on the weaning protocol. The number of patients weaned in hospital and decannulated was reduced in the post groups (both not significant).
Conclusions:
Utilizing RT protocols, daily rounds, and a weekly interdisciplinary meeting can improve quality of care and coordinate care effectively. The pilot study resulted in an improved mean LOS but was not statistically significant. Other positive results noted were increased teamwork, communication, accountability, and staff empowerment. Future studies should investigate more rigorous quality improvement methodologies and include larger sample sizes.
Get full access to this article
View all access options for this article.